

INTRODUCTION
Cardiovascular reactivity (CVR) is a responsiveness of the cardiovascular system to stressors. Excessive CVR is one of the critical risk factors of hypertension [1] and cardiovascular disease [2], and thus evaluation of CVR has been suggested as a clinical tool to predict the development of hypertension [3]. Cold pressor test (CPT) is often utilized in clinical settings to assess CVR via simulating sympathetic nervous system by immersing one hand in ice water during a short time (1-3 minute). The results from CPT are highly reproducible compared to other sympathoexcitatory tasks; as such, the CPT has been widely used to evaluate cardiac autonomic function and left ventricular function [4,5].
It is well known that aerobic exercise attenuates stress-related excessive CVR. A meta-analysis of the effect of acute aerobic exercise on blood pressure (BP) response to stressors showed significant mitigating effect in most studies [6]. Moreover, aerobic exercise training lowers heart rate (HR), rate pressure product (RPP), and systolic blood pressure (SBP) reactivity to psychological stress [7]. The suggested mechanism linked to the beneficial effect of aerobic exercise training on CVR is an increase in vasodilation by reduction in norepinephrine response and an increase in beta-2 receptor responsively [8].
The sympathetic nervous system (SNS) is repeatedly activated during each bout of aerobic or resistance exercise, so it could induce adaptation in the adrenergic system and may modulate SNS overactivity [9]. While the beneficial effects of aerobic exercise training on modulating CVR to sympathoexcitation have been consistently demonstrated, it remains unclear whether resistance training may also provide similar benefits. However, there is evidence to suggest that resistance training favorably reduces resting BP regardless of high- or low- intensity [10]. Other studies suggest that resistance training may also improve autonomic nervous function via enhancing parasympathetic tone [11,12], decrease resting cortisol levels [13], and induce faster HR recovery after peak exercise [14]. Considering the beneficial effects of resistance training on autonomic nervous function, similar effects on SNS can be expected in resistance training as well.
Indeed, Yoon et al. [15] reported that acute resistance exercise significantly attenuated SBP reactivity to CPT, but it is unknown whether there is favorable effect of regular resistance training on CVR. Although Sparding et al. [7] reported that SBP reactivity to psychological stress is alleviated after 6-week resistance training, it is unclear whether the same phenomenon will occur under physiological stressors.
Central blood pressure (cBP) and augmentation index (AIx) are independent predictors on cardiovascular diseases [16,17]. AIx is an index of wave reflection intensity, and is influenced by both peripheral and systemic arterial stiffness [18]. As arterial stiffness increases, transmission velocities of both forward-traveling waves from heart and reflected waves from periphery increase [17]. Consequently, this causes the reflected waves to arrive earlier in the central aorta and in turn augments cBP [19]. cBP is a marker directly reflecting the afterload on the heart, and thereby is more strongly related to cardiovascular diseases than brachial blood pressure (bBP) [20]. However, there are few studies used cBP and AIx as variables on CVR. During CPT, arterial stiffness is increased [21], and there is a greater augmentation in the cBP compared to the bBP [18]. To the best of our knowledge, whether the resistance training is capable to attenuate cBP and AIx under stress is not completely understood.
The purpose of this study was to investigate the effect of resistance training on CVR in young adults. To verify this, we hypothesized that resistance training could attenuate CVR to CPT in young adults. We expected this study to offer further evidences for recommending a resistance training program to individuals who had excessive CVR to stressors. In addition, we measured cBP and AIx as dependent variables with increased clinical significance. By verifying the effects of resistance training on these variables, we intended to expand existing research results.
METHODS
1. Subjects
Twenty-six subjects (male =16, female =10), aged between 18 and 30 years old, were recruited from the University of Seoul, Seoul, Korea. All subjects were sedentary healthy young adults whom had no medical history that could prevent them from attending the exercise program. The sedentary lifestyle was defined as not meeting the minimum requirement for the recommended physical activity levels (30 minutes a day, 3 days a week) for the last 3 months [22]. All subjects provided written informed consent prior to their study participation. The study protocol was approved by the Institutional Review Board (IRB) Committee of the University of Seoul/Seoul Medical Center (IRB number 2015-063).
2. Procedures
During the first visit, all subjects were completed PAR-Q (physical activity readiness questionnaire) to screen whether they should consult a doctor before participating in an exercise training program. During the second visit, the subjects were randomly assigned to either the resistance training group (RT, n =13, 5 females) or the control group (CON, n =13, 5 females), after which they underwent baseline assessments including anthropometric measures, maximal muscular strength via one-repetition maximum (1RM), and CVR to CPT. All subjects abstained from vigorous physical activity and alcoholic beverages for 24 hours, as well as smoking and caffeine for at least 3 hours prior to arriving to the laboratory for data collection. The measurements were performed again after 8 weeks of the intervention.
3. Resistance training program
The RT program was based on the previously published recommendations for healthy adults, in which the RT was performed twice a week, separated by at least 48 hours of rest between sessions, for a total of 8 weeks [22]. The RT program consisted of 2 sets of 9 exercises (chest press, lat pull down, machine shoulder press, machine preacher curl, leg press, leg extension, lying leg curl, torso rotation and machine back extension) targeting all major muscle groups. The RT program was carried out at 40-50% of 1RM for 15-25 repetitions per set during the first 4 weeks (weeks 1-4) and at 60-70% of 1RM for 10-15 repetitions per set during the last 4 weeks (weeks 5-8). The 1RM test was used to determine the training intensity, and it was measured at pre-training and after 1-4 weeks training and post-training, respectively. At the end of the 8-week intervention period, the attendance rate for the training program was 100%.
4. Outcome Measures
1) Anthropometric measures
Anthropometric data included body weight and height presented to the nearest 0.1 kg and 0.1 cm, respectively. Body mass index (BMI) was calculated as body weight (kg) divided by body height (m) squared (kg/m2). Percent body fat was measured using bioelectrical impedance analysis (InBody 3.0, Biospace, Seoul, Korea).
2) Maximal muscular strength
The 1RM test is a reliable indicator of maximal muscular strength. Although the actual 1RM test is the gold standard for evaluating maximal muscular strength, it may lead to muscle soreness and even serious injury to untrained participants [23]. Furthermore, untrained subjects are not always able to reach their actual 1RM [24]. To resolve these problems, an estimated 1RM testing, which is predicted based on the number of repetitions a participant could conduct with submaximal intensity, has been used in clinical settings. After performing the familiarization session including a light weight, the resistance was increased until the subjects could conduct only 7-10 repetitions. Thereafter, the prediction methods by O’Connor et al. [25] were used to determine an estimated 1RM using following equation: 1RM = repetition weight [1+0.025(repetitions)].
3) Resting heart rate and brachial blood pressure
Baseline bBP and HR were measured in the left arm in the supine position after a 5-minute rest using an automatic BP monitor (HEM-7080IC, Omron Healthcare Co., Kyoto, Japan). The measurements were performed twice, separated at least by 3 minutes, and the lowest value of the two was used. Rate pressure product (RPP), which is an indirect index of cardiac workload and myocardial oxygen consumption and predicts cardiac function [26,27], was calculated as [(HR×SBP)/100].
4) Resting central blood pressure and augmentation index
Baseline cBP and AIx were obtained by measuring radial artery pressure waveforms of the right wrist after 5 minutes of supine rest using applanation tonometry (Millar Instruments, Houston, Texas, USA). After sequential waveforms were recorded over 10 seconds period, central arterial pressure waveform and cBP were assessed by the SphygmoCor system (AtCor Medical, Sydney, Australia) using a generalized transfer function. To enhance the accuracy of measurements, only values whose quality index exceeded 80% were recorded, and then the average of the two values with a difference of less than 5% was used as data. Because AIx is affected by changes in HR, AIx at a HR of 75 beats/min (AIx@75) was additionally computed and adopted as a variable. As a result of test-retest reliability analysis for AIx measurements, intraclass correlation coefficient (ICC) was 0.997.
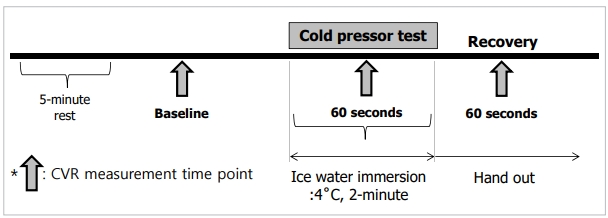
5) Cold pressor test
The CPT was performed by immersing a subject’s left hand in a 4°C water for 2 minutes [4], during which measurements of CVR were performed. HR, bBP, cBP, RPP, and AIx were measured at baseline, during the last 60 seconds of CPT, and during the last 60 seconds of the recovery period. Also, the magnitude of CVR is defined as ‘different value’, which was calculated as the difference between the resting value and the value obtained during the last 60 seconds of CPT. The overall design of CPT is shown in Fig. 1.
5. Statistical Analysis
All data were analyzed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Data were presented as means±standard deviations. To compare the difference in the variables with respect to subject characteristics, an independent samples t-test was used. To evaluate the changes of the factors related CVR during CPT between pre- and post-training in both groups, two-way analysis of variance (ANOVA) with repeated measures was used. Statistical significance was set at p< .05.
RESULTS
1. Changes of characteristics and muscular fitness
The characteristics of the subjects are shown in Table 1. Table 2 demonstrates the changes of characteristics including body composition and cardiovascular variables from pre- to post- intervention in both groups. There were no significant changes in all variables. Table 3 demonstrates the changes in maximal muscular strength of each of 9 exercises from pre- to post- intervention in both groups. There were significant increases in maximal muscular strength of 9 exercises (all p< .001) in the RT compared to the CON.
2. CVR changes during CPT
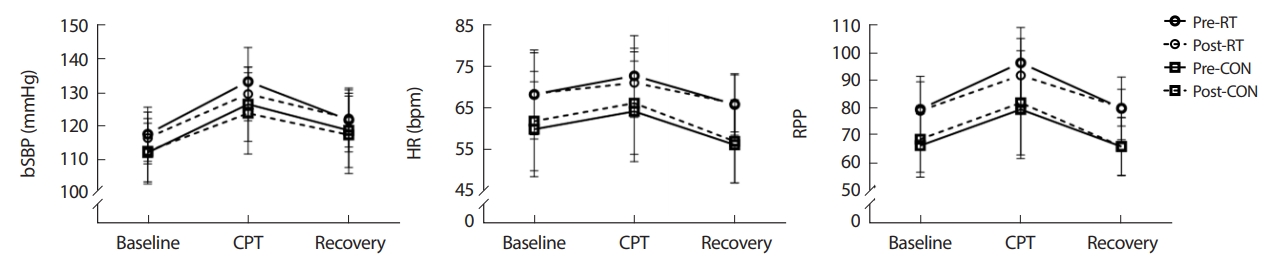
Fig. 2 demonstrates the changes in bSBP, HR and RPP measured at 3 time points (baseline, 60 seconds during CPT, 60 seconds during recovery) from pre- to post- intervention in both groups. There were no significant interaction effects in all variables between 2 groups and 3 time points in both pre- and post- intervention.
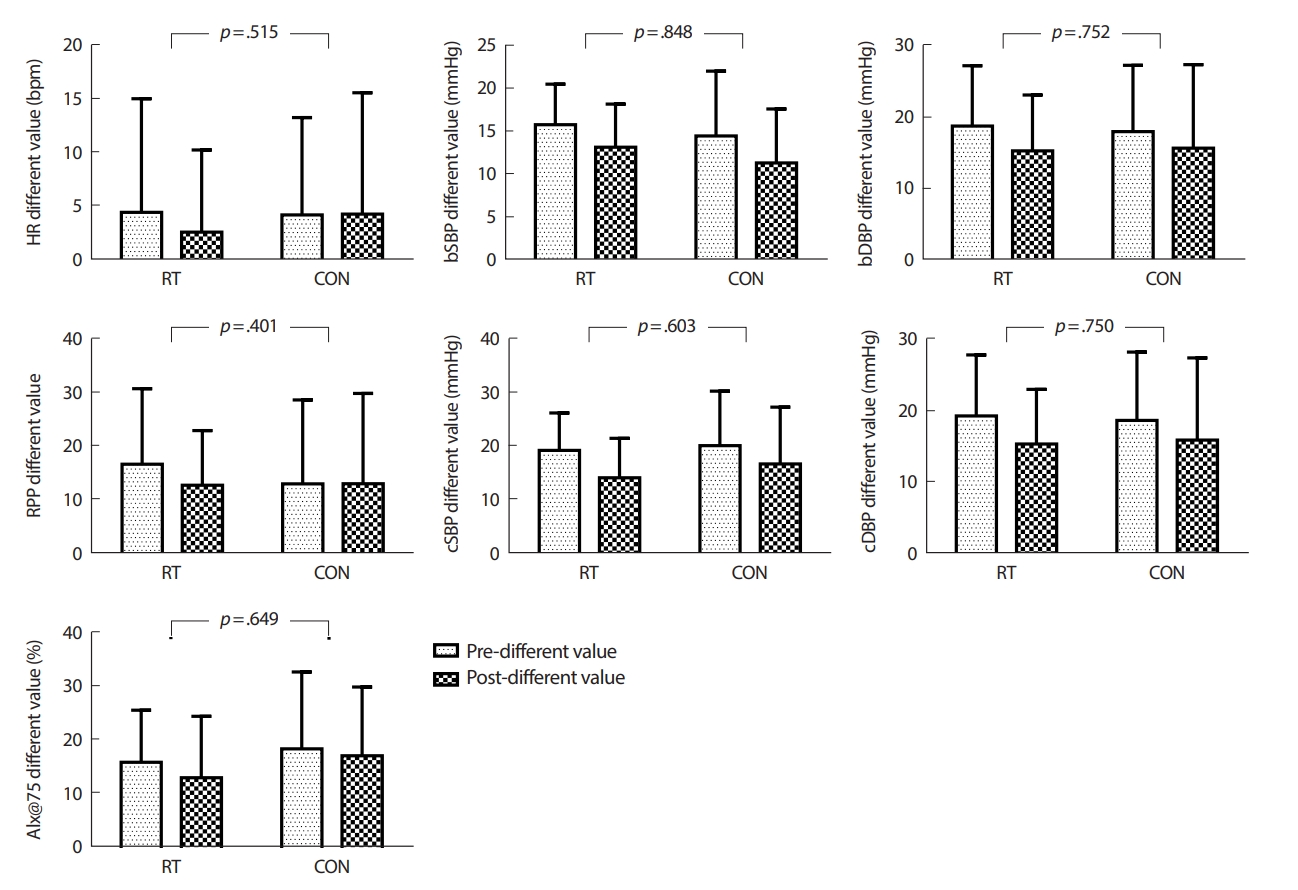
3. Magnitude of CVR
The magnitude of CVR is defined as ‘different value’, which was calculated as the difference between the resting value and the value obtained during the last 60 seconds of CPT. Fig. 3 demonstrates the changes in the different values of HR, bBP, RPP, cBP, and AIx@75 from pre- to post- intervention in both groups. There were no significant interaction effects in cardiovascular reactivity of all variables between 2 groups (RT and CON) and time (pre- and post- intervention).
DISCUSSION
The aim of this study was to investigate the effect of resistance training on CVR in young adults. However, in contrast to our hypothesis, resistance training did not have a mitigating effect on CVR including HR, bBP, RPP, cBP, and AIx during CPT in young adults.
The majority of the studies on CVR have mainly focused on the effect of aerobic exercise or training. It is well known that aerobic exercise or training attenuates CVR to both physiological and psychological stressors [6-8,28,29]. Like responses to stressors, acute exercise elicits augments in HR and BP by an increase in sympathetic activity with parasympathetic withdrawal. If the exercise is repeated, BP and HR responses to stressors are attenuated at equivalent workloads, which is called ‘the cross-stressor adaptation theory’ [30,31]. It means that adaptations to repetitive exercise stress can give rise to adaptations of the responses to other stressors. While there are studies supporting this theory, conflicting results have also been reported. Especially, the effects of resistance exercise or training on CVR to stressor have not been fully identified. Yoon et al. [15] reported that acute resistance exercise significantly alleviated SBP reactivity to CPT, however, it is unclear whether the same favorable effects will be elicited or maintained by regular resistance training.The aim of this study was to investigate the effect of resistance training on CVR in young adults. However, in contrast to our hypothesis, resistance training did not have a mitigating effect on CVR including HR, bBP, RPP, cBP, and AIx during CPT in young adults.
Spalding et al. [7] studied that the effects of 6 weeks of aerobic training and resistance training on CVR to psychological stressor in young adults with normal BP. Similar to our study, there were no significant reducing effects of resistance training on bDBP, HR and RPP reactivity to stressor. However, contrary to our results, resistance training significantly reduced bSBP reactivity to stressor compared to aerobic training. These disparate results may be derived from different stressors utilized by our group and their group (CPT vs. mental arithmetic, respectively). While psychological tasks cause relatively higher augments in SBP and HR by increasing stimulation of beta-adrenergic receptors, physiological tasks elicit a relatively higher augment in DBP by increasing stimulation of alpha-adrenergic receptors, which leads to peripheral vasoconstriction [29]. Indeed, the magnitude of DBP reactivity to CPT was higher than that of SBP reactivity in our study, but the magnitude of SBP reactivity to mental arithmetic was higher than that of DBP reactivity [7]. Furthermore, our resistance training program consisted of 2 sets of 9 exercises during 8 weeks (16 sessions) was carried out at 40-50% of 1RM for 15-25 repetitions per set during 1-4 weeks and at 60-70% of 1RM for 10-15 repetitions per set during 5-8 weeks. On the other hand, Spalding et al. [7] used the 6 weeks program which carried out at 60-80% of 1RM for 3 sets three times a week (18-30 sessions). It means that the difference of training protocol may be the cause of these disparate results. Therefore, further studies are needed to determine the effects of various methods of resistance training on various physiological tasks.
Sloan et al. [30] studied that the effects of 12 weeks of aerobic training and resistance training on CVR to psychological and physiological mixed stressors. Their mixed stressors consisted of simulated public speaking as the first stressor and mental arithmetic and stroop task on tilt table with moving to the 70° head-up position as the second mixed stressor. In this study, while aerobic training only increased aerobic capacity, both aerobic training and resistance training did not attenuate CVR on mixed stressors [30]. Not only is the result consistent with ours, but it is conflict with ‘the cross-stressor adaptation theory’ explained above. According to the previous research, maximum CVR was induced in isometric hand grip test, and maximum gender difference in CVR was induced in CPT [32]. Accordingly, additional studies are needed to investigate whether the effects of resistance training on various single physiological stressors such as CPT and isometric hand grip test. Especially, CPT has more reproducibility than other sympathoexcitatory tasks [5], and it was recently reported that bSBP reactivity to CPT was positively associated with risks for future hypertension [1]. Due to these merits of CPT, the effects of various exercise training modes on CVR to CPT would be more beneficial. To sum up, ‘the cross-stressor adaptation theory’ has not yet come to a definite conclusion. There are still more issues, which need to be clarified, including different effects following exercise modes, stress task types and participants’ characteristics.
Our study has some limitations. Firstly, young adults were only selected as our subjects. Individuals whose bSBP augments by 25 mmHg or more or whose bDBP augments by 20 mmHg or more are regarded as hyperreactive to CPT [4]. All our subjects were young and healthy, and none of them had hyperreactivity to CPT. Therefore, further studies including subjects who had hyperreactivity to CPT are required for verification of the effects of resistance training on CVR. Secondly, the sample size of our subjects was small. So, further studies with larger sample sizes are necessary to increase the external validity of the present. Lastly, we could not consider possible gender differences regarding CVR. So, further studies are needed to investigate the gender differences in effects of resistance training on CVR. We expect that adequate frequency, intensity, time, and type of resistance exercise program for people with hyperreactivity to stress will be established through these studies.
CONCLUSION
The purpose of the present study was to investigate the effect of resistance training on CVR in young adults. We expected this study to offer further evidences for recommending a resistance training program to individuals who had excessive CVR to stressors. The results from this study suggest that resistance training is not able to attenuate CVR including HR, bBP, RPP, cBP, and AIx during CPT in young adults. Considering the limitations of our study, further studies are necessary to verify whether ‘the cross-stressor adaptation theory’ is also applied to resistance training.