운동 전 온열처치가 저항성 운동 후 근육 손상 지표에 미치는 영향
Abstracts
PURPOSE
This study aimed to investigate the effect of pre-exercise heat pack treatment on muscle activity and markers of muscle damage after exercise-induced damage.
METHODS
Ten healthy male university students were tested for 3 weeks. They were exposed to three conditions (non-warm-up exercise, warm-up exercise, and heat pack treatment) before exercise. The experiment was conducted at 1-week intervals for every partici-pant. The warm-up exercise was performed by combining a modified active warm-up with a cycle ergometer and an isokinetic dynamometer. The main exercise, which modified the exercise-induced muscle damage protocol, was conducted by flexing and extending the knee joint using an isokinetic dynamometer. The heat pack treatment before the exercise involved moist heat application for 20 min.
RESULTS
The changes in blood muscle fatigue markers and blood muscle damage markers were not significantly different between the groups (α>.05). However, significant differences were observed in the time immediately after exercise, 10-min recovery, 30-min recovery, and 60-min recovery (p<.05). A statistically significant difference was observed in the change in pain in the heat pack treatment group (p<.05).
CONCLUSIONS
Heat pack treatment for 20 min before exercise did not minimize the muscle damage markers and fatigue markers following exercise-induced damage, but reduced immediate muscle soreness. Use of heat pack treatment was associated with a change in muscle activity and improvement in certain aspects of muscle soreness.
Keywords: Heat pack treatment, Muscle damage
색인어: 온열처치, 근육손상
서 론
스포츠 상해의 회복을 위해서는 많은 시간과 비용 그리고 처치에 따른 어려움이 동반되므로 경제적인 측면과 함께 의학적인 측면이 고려되는 예방적인 전략이 요구된다[ 1]. 스포츠 상해 예방을 위하여 일반적으로 적용되는 방법은 적절한 준비운동의 수행이며[ 2– 5], 크게 두 가지로 구분된다[ 4]. 한 가지는 자발적인 신체활동(조깅, 사이클링 등)을 통하여 체온 상승을 유도하는 능동적 준비운동(active warm-up)이며[ 6– 9], 다른 하나는 외부요인(온수샤워, 온열팩 등)에 의해 근육 온도의 상승이나 심부체온 상승이 일어나 는 수동적 준비운동(passive warm-up) 방법이다[ 7, 10– 12]. 선행연구에 따르면 저항성 운동 전 20분간의 에르고미터 사이클 준비운동을 실시한 그룹에서는 근육 통증(muscle soreness)을 예방하는 데 효과가 있다고 나타났으며[ 8], 지연성 근육통(delayed onset muscle soreness)을 예방하기 위해 조깅, 사이클과 같은 준비운동을 실시해야 한다고 보고되었다[ 9]. 또한 온수샤워, 온열팩 등과 같은 외적인 수단에 의한 수동적 준비운동은 격렬한 운동으로 유발된 근육손상(muscle damage)을 보호하는 데 효과적이다[ 11, 12]. 일반적으로 만성 손상 시 적용되는 온열요법은 통증 제거, 근육 및 인대의 유연성 증가 효과가 있으며, 환자의 기능적인 상태를 최상의 컨디션으로 만드는 데 목적이 있다[ 13– 16]. 뿐만 아니라, 조직 온도를 상승시키고, 국소적용부위의 혈관확장을 통하여 혈류량을 증가시키며, 교원 조직의 물리적 변화와 대사 활동 증가, 신경 반응 변화, 근골격계 활동의 변화를 야기시키는 것으로 보고된다[ 15– 20]. 이러한 관점에서 온열요법은 격렬한 운동으로 인해 야기된 근육손상을 회복시키는 방법으로 적용될 수 있다[ 21]. 근육손상(muscle damage)은 급성 근육통(acute muscle soreness)[ 22] 및 지연성 근육통(delayed onset muscle soreness)[ 22, 23]을 동반하며 근기능[ 24], 관절가동범위(range of motion)[ 25], 최대 수의근력[ 25] 감소를 일으킨다. 특히 고강도 근력운동으로 유발된 근육손상은 고유 수용성 감각(proprioception)을 감소시켜 힘의 인식과 동작의 움직임에 변화[ 26, 27]를 가져오기 때문에 근육손상의 회복을 위한 처치 방법과 관련된 다양한 연구가 진행되고 있다[ 21, 28]. 이전 연구에 따르면 운동 전 온열 적용은 원심성 수축 운동(eccentric contraction exercise)으로 유발된 근육 손상을 보호하는 데 효과적이라고 보고하였다[ 11, 12]. 또한, 온열 적용을 받지 않은 그룹과 비교했을 때 온열 그룹에서는 운동 후 1일에서 4일 사이의 최대 수의근력이 유의하게 증가하였고 근육 통증이 낮은 결과를 보였다[ 12]. 운동 전 온열 적용은 근육의 온도가 상승함에 따라 근수축 속도에 이점이 있는 반면에, 근육이 수축하는 동안 힘의 산출량이 증가함으로써 근피로율 또한 증가하게 되기도 한다[ 29]. 따라서, 온열 적용이 근활성도 및 근육손상 지표에 미치는 영향을 알아보기 위하여 원심성 수축과 구심성 수축(concentric contraction)으로 이루어진 운동을 적용하는 것이 효율적이라 제안된다. 본 연구에서는 온열팩을 이용한 일회성 처치의 효과를 입증하고, 경기력 향상 및 스포츠 상해 예방을 위한 준비운동을 보다 편리하고 전략적으로 효과적인 처치를 할 수 있도록 근활성도(중앙주파수: medi-an frequency, MDF)와 혈액학적 분석(creatine kinase, CK), (lactate de-hydrogenase, LDH)을 통해 온열 적용에 관한 모델링을 제시하고자 한다. 따라서, 본 연구의 목적은 저항성 운동 전 일회성 온열 처치가 근활성도, 근육통증, CK, LDH와 같은 근육손상 지표에 미치는 영향을 조사하는 것이다.
연구 방법
1. 연구대상
본 연구는 건강한 20대 남자 대학생 10명(연령 23.60±1.26 years, 신장 174.02±4.16 cm, 체중 77.67±10.72 kg, 체지방률 21.16±4.56%)을 대상으로 실시하였다. 대상자 선정과 관련하여 American College of Sports Medicine (ACSM)과 American Heart Association (AHA) 가이드라인[ 30]에 따라 중강도 운동을 주 5회, 30분 이상 참여하거나 고강도 운동을 주 3회, 20분 이상 참여하는 신체적으로 활동적인 사람을 선정하였으며, 최근 6개월 이내에 약물을 복용하지 않은 사람, 화상, 감각장애 및 중추신경손상, 말초신경손상이 없는 사람으로 한정하였다. 실험 기간 동안 타당성 있는 실험 결과를 얻기 위해 실험 전 과도한 신체활동을 하지 않도록 요구하였으며, 실험 전날 8시간 이상의 공복을 유지하도록 하였다. 모든 대상자들은 실험 시작 전 실험에 대한 제반 사항 및 진행 절차, 그리고 실험 중 발생할 수 있는 위험요소에 대해서 자세한 설명을 들었으며, 본인이 원하지 않는 경우 언제라도 자유롭게 본 실험의 참가를 그만둘 수 있다는 사항들을 포함한 실험 동의서를 작성하였다.
2. 실험절차
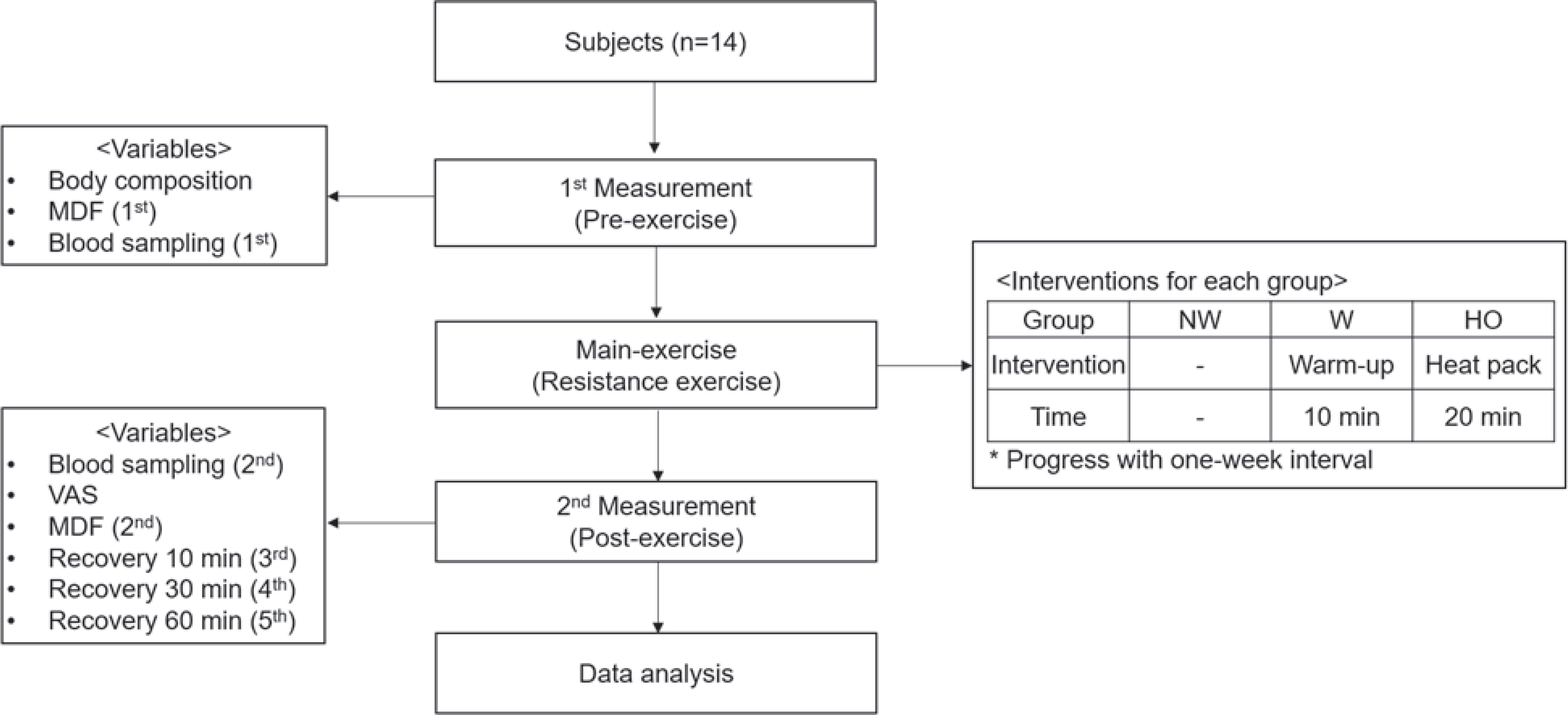
모든 대상자들은 실험 30분 전에 실험실에서 대기하면서 적응하는 시간을 갖도록 하였고 실험실 내의 온도(23-25°C)와 습도(50-60%)를 일정하게 유지하였다. 동일한 피험자 10명을 대상으로 3회(NW, W, HO)에 걸쳐 반복적으로 실험을 실시하였다( Table 1).
Table 1.
Classification of subjects
|
Group |
Group description |
|
NW |
Non warm-up and main exercise and measurement |
|
W |
Warm-up and main exercise and measurement |
|
HO |
20 min heating and main exercise and measurement |
실험실 방문 첫날, 각 대상자들의 신체 조성 검사를 실시하였다. 각 조건별 실험 진행 시 5회에 걸쳐 혈액(운동 전, 운동 직후, 운동 후 회복 10분, 회복 30분, 회복 60분)을 채취하였으며, 2회에 걸쳐 표면 근전도(운동 전, 운동 직후)를 측정하였다. 또한, 운동 직후 피험자가 주관적으로 느끼는 근육 통증 수준을 측정하였다. 이때, 선행 실험이 다음 실험에 미치는 영향을 극소화하기 위해 3회의 실험 간격을 1주일 이상 두어 진행하였다. 구체적인 실험절차는 Fig. 1과 같다.
Fig. 1.
Fig. 1.
3. 측정항목 및 방법
1) 신체 조성 검사
신체 조성 검사는 전기 저항법에 의해서 측정되는 체성분 분석기 (Body Composition Analyzer [Venus-5.5, Jawon Medical, Seoul, Korea])를 이용하였으며, 가벼운 운동복을 입은 상태에서 신장과 체중, 체지방률, 제지방량을 측정하였다[ 31, 32].
2) 표면 근전도 측정
표면 근전도의 측정은 건식 전극방식의 무선 근전도 측정장치(Tri-gno wireless system, Delsys Inc., Boston, USA)를 이용하여 무선 Trigno sensor에 일회용 전용패치를 부착하여 피험자의 넙다리곧은근(rectus femoris)과 가쪽넓은근(vastus lateralis) 근육의 가장 활성화되는 근복(muscle belly)에 수평방향으로 부착하여 측정하였다[ 33]. 무선 Trigno sensor 전극을 부착하기 전에 피부저항을 최소화하기 위해 대상 부위를 면도한 후 소독용 알코올로 청결하게 닦아준 다음 완전히 마른 다음 전극을 부착( Table 2)하였다[ 34]. 근전도 신호는 sampling rate를 4,000 Hz로 하여 2개의 무선채널을 이용하여 수집하였다. 근전도 신호의 저장과 분석은 signal acquisition and analysis software (Delsys Inc., EMGwork 4.0, USA)를 이용하였다.
Table 2.
EMG electrode attachments
|
Muscle |
Attachment part |
|
Rectus femoris |
Middle thigh front side (middle side of the iliac crest and knee) |
|
Vastus lateralis |
Knee upwards of about 3-5 cm diagonal at the point facing outwards |
3) 통증 수준 평가
통증 수준의 평가는 100 mm 시각적 상사 척도(visual analogue scale, VAS)를 사용하였으며, 환자가 주관적으로 느끼는 통증 정도를 0-10 cm의 선에 표시하는 방법이다(0 cm: 통증 자각증상 없음, 10 cm: 극심한 통증 발생)[ 35]. VAS는 검사-재검사 신뢰도(r=.99)와 측정자 간의 신뢰도(r=1.00)가 매우 높은 검사 방법이다[ 36].
4) 혈액 채취 및 분석
혈액의 채취는 운동 전 안정 시와, 운동 직후, 운동 후 회복 10분, 회 복 30분, 회복 60분에 실시하여 각 실험 당 5차례의 채혈을 실시하였다. 혈액은 각각의 시기마다 5 cc씩 22 gauge needle을 이용하여 전완 정맥(antebrachial vein)에서 채혈하였다. SST tube와 NAF tube에 채혈한 혈액은 원심분리기를 이용하여 3,000 rpm으로 10분간 원심 분리한 뒤 −80°C 냉동고에 보관하였으며, 각 분석 kit에 맞게 CK, LDH를 분석하였다[ 37].
5) 일회성 저항성 운동
본 연구의 준비운동 프로토콜은 Nosaka & Clarkson [ 38]의 연구에서 사용된 active warm-up을 변형하여 사이클 에르고미터 운동과 결합( Table 3)하였으며, 준비운동이 본 운동에 영향을 주지 않도록 강도를 설정하였다. 본 운동 프로토콜은 Eduardo da Silva et al. [ 39]의 근손상유도 프로토콜을 변형( Table 3)하였다. 등속성 운동 장비(Cybex770, Cybex division of lumax, NY, USA)를 이용하여 무릎 굽힘근과 폄근의 원심성 수축과 구심성 수축을 이용한 인위적인 최대 운동을 통해 근육손상을 유발시켰다.
Table 3.
Warm-up and main exercise protocol
|
Type |
Protocol |
|
Passive warm-up |
20 min heating before main exercise |
|
Active warm-up |
Cycle ergometer 6 min 40 s (50 RPM), Cybex knee exercise(velocity 120, rep 100) 3 min 20 s |
|
Main exercise |
Muscle damage protocol: Cybex knee exercise (8 set)
1) Concentric (extensors, flexors), rep (3), velocity (60), Interval (15 s)
2) Concentric (extensors, flexors), rep (20), velocity (60), Interval (60 s)
3) Concentric and eccentric (flexors), rep (3), velocity (60), Interval (15 s)
4) Concentric and eccentric (flexors), rep (20), velocity (60), Interval (60 s)
5) Concentric and eccentric (extensors), rep (3), velocity (60), Interval (15 s)
6) Concentric and eccentric (extensors), rep (20), velocity (60), Interval (60 s)
7) Concentric (extensors, flexors), rep (3), velocity (60), Interval (15 s)
8) Concentric (extensors, flexors), rep (20), velocity (60), Interval (60 s) |
6) 일회성 온열 처치
일회성 온열 처치를 위해 온도 조절 기능이 있는 항온수조(KRS-12PD, Karis, Korea)에 의해 71-79°C로 유지된 온습포를 사용하였다 [ 40]. 온습포 표면을 수건으로 감싸고 대퇴부 전면에 밀착시켜 원형으로 말아서 적용하였으며 비접촉식 적외선 온도계(Smart Sensor Pro AS550, Intellisafe. Co., USA)를 이용하여 온습포 적용 전과 후의 체표면 온도를 측정하면서 20분간 적용시켰다.
4. 자료 처리 방법
본 연구에서 얻어진 모든 자료는 Window용 SPSS/PC 20.0 통계 프로그램을 이용하여 기술 통계(평균과 표준편차)를 산출하였다. 처치 방법에 따른 집단 간의 차이는 반복 측정된 이원분산분석(two-way ANOVA with repeated measures)을 실시하였으며, 유의한 차이가 있는 경우 사후분석을 위해 least significant difference (LSD)를 이용하였다. 또한, 본 운동 후 그룹 간의 통증 수준을 비교하기 위해 일원분산분석(one-way ANOVA)을 실시하였으며, 유의한 차이가 있는 경우 사후분석을 위해 LSD를 이용하였다. 근전도는 시기간 유의한 차이가 있는 경우 대응 표본 t-test를 이용하여 검증하였다. 모든 통계적 유의수준은 α=.05로 설정하였다.
결 과
1. 저항성 운동 후 근활성도 변화
세 그룹 모두 가쪽넓은근의 변화는 나타나지 않았다. 하지만, 근피로도가 높아짐에 따라 NW 그룹에서 넙다리곧은근이 유의하게 감소하였다( p <.001) ( Table 4).
Table 4.
Change of MDF after exercise-induced muscle damage
|
Group |
Vastus lateralis (Hz)
|
Rectus femoris (Hz)
|
|
Pre |
Post |
Pre |
Post |
|
NW |
69.21 ± 12.78 |
68.27 ± 10.66 |
58.94 ± 7.12 |
53.13 ± 8.01*
|
|
W |
75.54 ± 16.43 |
73.43 ± 12.45 |
61.45 ± 11.88 |
62.43 ± 13.44 |
|
HO |
75.54 ± 16.43 |
70.89 ± 11.70 |
60.98 ± 5.73 |
64.61 ± 2.65 |
2. 저항성 운동 후 근육통증의 변화
저항성 운동 후 각 그룹별 VAS 값을 살펴본 결과, NW 그룹 8.25±0.82, W 그룹 8.25±0.86, HO 그룹 7.4±0.84로 나타났다. NW, W 그룹에 비해 HO 그룹이 유의하게 낮게 나타났다( p <.05) ( Table 5).
Table 5.
Change of VAS after exercise-induced muscle damage
|
Group |
VAS (cm) |
F |
p
|
|
NW |
8.25 ± 0.82*
|
3.396 |
.048 |
|
W |
8.25 ± 0.86†
|
|
|
|
HO |
7.40 ± 0.84 |
|
|
3. 저항성 운동 후 근육손상 지표의 변화
각 그룹별 실험은 1주일 간격으로 진행하였으며, 본 운동 전 조건을 다르게 한 저항성 운동 후 혈중 CK, LDH 변화는 Table 6에 나타나 있다.
Table 6.
Change of muscle damage markers
|
Variables |
Group |
Pre-Ex. |
Post-Ex. |
Recovery 10 min |
Recovery 30 min |
Recovery 60 min |
|
CK (IU/L) |
NW |
191.0 ± 37.0 |
199.7 ± 36.9*
|
198.3 ± 38.0*
|
196.2 ± 35.0 |
196.3 ± 39.0 |
|
|
W |
192.6 ± 44.3 |
207.4 ± 47.4*
|
198.5 ± 47.9*,†
|
196.8 ± 46.3†
|
196.3 ± 48.8†
|
|
|
HO |
193.4 ± 44.4 |
203.0 ± 48.8*
|
194.8 ± 48.3†
|
186.1 ± 43.1*,†‡
|
189.3 ± 45.9†,‡
|
|
LDH (IU/L) |
NW |
202.8 ± 28.7 |
280.9 ± 72.4*
|
247.8 ± 74.1*
|
274.7 ± 104.9*
|
265.7 ± 102.9*
|
|
|
W |
203.2 ± 31.6 |
227.4 ± 37.7*
|
249.0 ± 70.1*
|
209.0 ± 47.8†‡
|
210.1 ± 61.7 |
|
|
HO |
201.9 ± 30.4 |
221.6 ± 33.7*
|
233.1 ± 40.4 |
201.0 ± 30.7†
|
204.5 ± 32.4†
|
4. 저항성 운동 후 CK의 변화
세 그룹 모두 안정 시보다 운동 후 혈중 CK 농도가 유의하게 증가하였다(p <.01). NW 그룹에서 안정 시를 기준으로 운동 직후와 회복 10분에서 유의한 차이를 보였다(p <.05). W 그룹에서는 안정 시를 기준으로 운동 직후와 회복 10분에서, 운동 직후를 기준으로 회복 10분, 30분, 60분에서 유의한 차이를 보였다(p <.05). 그리고 HO 그룹에서는 안정 시를 기준으로 운동 직후와 회복 30분에서, 운동 직후를 기준으로 회복 10분, 30분, 60분에서의 차이가 유의하게 나타났으며(p <.05), 회복 10분을 기준으로 회복 30분과 60분에서 통계적으로 유의한 차이를 보였다(p <.05).
5. 저항성 운동 후 LDH의 변화
세 그룹 모두 안정 시보다 운동 후 혈중 LDH 농도가 유의하게 증가하였다(p <.01). NW 그룹에서 안정 시를 기준으로 운동 직후, 회복 10분, 30분, 60분에서 통계적으로 유의한 차이를 보였으며(p <.05), W 그룹에서는 안정 시를 기준으로 운동 직후와 회복 10분에서 시기 간 유 의한 차이가 나타났다(p <.05). 또한, 회복 30분에서는 운동 직후와 회복 10분과 비교하여 유의한 차이가 있었다(p <.05). HO 그룹에서는 안정 시를 기준으로 운동 직후에 통계적으로 유의한 차이를 보였으며(p <.05), 운동 직후를 기준으로 회복 30분과 60분에 통계적으로 유의한 차이를 보였다(p <.05).
논 의
본 연구는 근손상 유도 프로토콜을 적용 후, 온열 처치가 근활성도와 근피로에 미치는 영향을 알아보고자 하였다. 준비운동은 체온 상승에 의한 파워 증대, 호흡 순환계의 적응력 향상, 신경기능의 항진, 신체 각 관절의 유연성 증가 등 다양한 이점과 운동 시 발생할 수 있는 상해 예방 효과가 있지만[ 2, 3, 5, 6, 41], 준비운동의 효율성에 대해서는 논란의 여지가 많다. 선행 연구를 살펴보면, 10분 동안 준비운동을 시행하였을 때 지연성 근육통을 감소시켰지만 그 차이는 크지 않은 것으로 보고되었으며[ 42], 15분 동안의 준비운동은 신장성 운동 후 근육통을 완화시키는 데 효과가 있는 것으로 나타났다[ 43]. 더 오랜 시간 준비운동을 시행하였을 때 지연성 근육통 예방에 대한 더 큰 효과를 갖는다고 하였다[ 44]. 온열팩 처치는 passive warm-up의 형태로 제시되며, 40°C 온열패드를 20분 동안 적용시키는 것이 온열요법의 일반적인 형태로 알려져 있다[ 45]. 사실, 온열은 수천 년 동안 치료에 사용되어져 왔는데, 즉각적인 통증 완화를 제공하며, 손상 후 순환을 증가시켜 치유 과정을 촉진시킨다[ 17]. 이러한 이유 때문에 온열은 연부조직 손상으로 인한 통증뿐 아니라 관절 및 근육의 여러 형태의 통증에서 대중적으로 사용되고 있다[ 46]. 열의 또 다른 효과는 혈액순환을 증가시키는 기능이다. 통각수용기와 TRPV 같은 수용체들은 열에 반응하여 혈류를 증가시킨다. 열에 대한 초기 반응은 순환을 증진시키는 것과 관련이 있는 물질 P와 칼시토닌 G 관련 펩타이드의 연결을 해제시키는 감각신경을 통해 매개한다. 혈류순환의 증가는 조직을 열로부터 보호하고 손상된 조직의 회복에 필수적이다[ 47]. 본 연구와 유사한 결과를 보인 선행연구에 따르면 만성요통환자(chronic low back pain)에게 2시간 동안 온열요법을 적용한 결과, 척추세움근(erector spinae muscles)의 근활성도와 통증을 감소시킨 것으로 나타났으며 심리적인 요인의 변화에도 기인한다고 하였다[ 48]. 또한, Eisuke Hiruma et al. [ 45]의 연구에서는 20분 동안의 온열요법이 반복적인 종아리 근육 최대운동에서 유발된 지연성 근육통을 최소화시키지는 못하지만 즉각적으로 근육통을 줄이는 데에 도움이 된다고 보고하였다. 근손상 유도 프로토콜 적용 후 VAS를 이용한 대퇴부의 통증을 조사한 결과를 살펴보면, 온열팩을 적용한 그룹이 준비운동을 하지 않은 그룹과 준비운동을 한 그룹보다 유의하게 낮게 나타났다( p <.05). 운동 직후 회복기 1시간 동안 관찰하였기 때문에 지연성 통증의 감소 여부는 판단할 수 없지만 근피로 유발 후 즉각적으로 발생하는 근육통이 감소한 것으로 나타나 운동 전 온열 적용이 근육통 예방을 위해 현장에서 적용할 수 있음을 시사한다. 그러나 가장 일반적이고 보편화되어 있는 VAS만을 이용하여 통증을 조사하였기 때문에 결과를 일반화시키기에 제한이 따를 것으로 보인다. 또한, Lewis et al. [ 48]은 온열요법을 받은 그룹에서 심리적인 요인이 통증에 대한 값에 크게 작용하는 것으로 여겨지기 때문에 통증의 변화를 조사할 수 있는 객관적인 평가방법이 요구되는 것으로 보인다. 본 연구에서는 체온 상승 효과를 기대할 수 있는 준비운동 그룹과 온열 처치 그룹에서 MDF 값이 증가하였으며, 준비운동 미실시 그룹에서 넙다리곧은근의 유의한 감소가 나타났다. 근전도는 골격근의 기능적인 특성을 평가하기 위해서 비침습적으로 사용되며 편리하게 근육의 전기적 활동을 스펙트럼으로 분석할 수 있다[ 49]. Pereira et al. [ 50]의 연구에서 상완이두근에 극초단파를 16분 적용한 결과, 등척성 수축력과 근활성도는 감소하였고 MDF 값은 증가하였다. 증가된 MDF 값은 근피로가 감소하는 것을 의미하며[ 51], 이는 근육의 온도 상승에 따라 혈관확장이 일어나고 혈류량이 증가하여 근육에 혈액과 영양공급이 기인한 결과이다[ 52]. 또한, 근수축에 대한 운동 단위(motor unit)의 발화율이 증가하게 되어 근수축이 효율적으로 일어났기 때문일 것이다[ 53]. 본 연구에서의 준비운동 그룹과 온열요법 그룹에서 근피로도 감소의 요인으로 사료된다. 따라서, 근피로도 감소에서 준비운동과 온열요법 중재의 효과를 확인할 수 있었으며, 임상적 근거 자료로 활용될 수 있을 것으로 예측된다. 대부분의 선행 연구는 주로 운동 후 회복기에 온열 및 치료 적용에 대한 비교 연구를 보고하였다. Rodrigues et al. [ 54]과 Machado et al. [ 55]의 연구에서는 LDH와 CK 값이 운동 후 회복기 24-72시간에 가장 높아지며 다양한 변화 추이를 보인다고 보고하였다. 본 연구에서는 세 그룹 모두 운동 직후 LDH와 CK값이 증가하였지만, 회복에 대한 양상은 다르게 나타났다. 운동 전과 비교했을 때, CK는 세 그룹 모두 회복 60분이 경과한 시점과 유의한 차이가 없었다. 하지만, LDH는 준비운동 미실시 그룹에서만 안정 시보다 유의하게 높은 상태가 지속되어( p <.05), 온열 적용이 LDH 값의 증가를 억제시키는 것으로 사료된다. 한 선행연구에 따르면 근손상 유도 프로토콜을 적용 후 저출력 레이저 치료(low level laser therapy, LLLT)를 적용하였을 때, 회복기 72시간 시점에 CK 값이 감소하였다[ 56]. 선행연구를 바탕으로 살펴보았을 때, 정확한 연구결과를 도출하기 위해 회복기 72시간 이후까지 근피로 지표의 변화 추이를 관찰할 필요가 있는 것으로 판단된다. 후속 연구에서 온열패드의 온도별, 시간별, 국소적 적용 여부와 외부환경 조절로 인한 전체 체온 상승을 유도 여부를 구분 지을 수 있는 비교 연구가 진행된다면 운동 전 처치를 통해 기대할 수 있는 여러 긍정적인 효과를 얻을 수 있을 것이라 예측된다.
결 론
경제적이고 사용이 편리한 온열 처치를 운동 전 적용하는 것만으로 운동으로 야기된 근피로로 인한 통증 조절에 효과가 있는 것으로 보이고 이는 상해 예방이나 경기력 향상을 위한 측면에서 간편한 프로그램 제시하는 데 도움이 될 것이다. 또한 근육이 최적의 상태로 운동 수행력을 증대시키기 위하여 온열팩 처치의 적용 시간이나 온도 측면에서 적용 방법을 고려하여 사용한다면 보다 안전하고 효율적으로 준비운동 전략을 수립할 수 있을 거라 제안한다.
REFERENCES
1. Parkkari J, Kujala UM, Kannus P. Is it possible to prevent sports injuries? Sports Med. 2001;31(14):985-95.   4. McGowan CJ, Pyne DB, Thompson KG, Rattray B. Warm-up strategies for sport and exercise: mechanisms and applications. Sports Med. 2015;45(11):1523-46. 5. Soligard T, Nilstad A, Steffen K, Myklebust G, Holme I, et al. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med. 2010;44(11):787-93. 6. Bishop D. Warm up II. Sports Med. 2003;33(7):483-98. 7. Cè E, Margonato V, Casasco M, Veicsteinas A. Effects of stretching on maximal anaerobic power: the roles of active and passive warm-ups. J Strength Cond Res. 2008;22(3):794-800. 9. Szymanski DJ. Recommendations for the avoidance of delayed-onset muscle soreness. Strength Cond J. 2001;23(4):7. 10. Bishop D. Warm up I. Sports Med. 2003;33(6):439-54. 11. Saga N, Katamoto S, Naito H. Effect of heat preconditioning by microwave hyperthermia on human skeletal muscle after eccentric exercise. J Sports Sci Med. 2008;7(1):176.  12. Nosaka K, Muthalib M, Lavender A, Laursen PB. Attenuation of muscle damage by preconditioning with muscle hyperthermia 1-day prior to eccentric exercise. Eur J Appl Physiol. 2007;99(2):183-92. 13. Grana W. Physical agents in musculoskeletal problems: heat and cold therapy modalities. Instr Course Lect. 1993;42:439-42. 14. Petrofsky JS, Laymon M, Lee H. Effect of heat and cold on tendon flexibility and force to flex the human knee. Med Sci Mon Int Med J Exp Clin Res. 2013;19:661. 15. Malanga GA, Yan N, Stark J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad Med. 2015;127(1):57-65. 16. Petrofsky J, Berk L, Bains G, Khowailed IA, Lee H, et al. The efficacy of sustained heat treatment on delayed-onset muscle soreness. Clin J Sport Med. 2017;27(4):329-37. 17. French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. Superficial heat or cold for low back pain. Cochrane Database Syst Rev. 2006;(1):CD004750. 18. Petrofsky JS, Lawson D, Suh HJ, Rossi C, Zapata K, et al. The influence of local versus global heat on the healing of chronic wounds in patients with diabetes. Diabetes Technol Ther. 2007;9(6):535-44. 19. Laymon M, Petrofsky J, McKivigan J, Lee H, Yim J. Effect of heat, cold, and pressure on the transverse carpal ligament and median nerve: a pilot study. Med Sci Mon Int Med J Exp Clin Res. 2015;21:446. 20. Kain J, Martorello L, Swanson E, Sego S. Comparison of an indirect tri-planar myofascial release (MFR) technique and a hot pack for increasing range of motion. J Bodyw Mov Ther. 2011;15(1):63-7. 21. Kim K, Monroe JC, Gavin TP, Roseguini BT. Local heat therapy to accelerate recovery after exercise-induced muscle damage. Exerc Sport Sci Rev. 2020;48(4):163-9. 23. Cheung K, Hume PA, Maxwell L. Delayed onset muscle soreness. Sports Med. 2003;33(2):145-64. 24. Clarkson PM, Hubal MJ. Exercise-induced muscle damage in humans. Am J Phys Med Rehabil. 2002;81(11):S52-S69. 25. Lavender AP, Nosaka K. Changes in fluctuation of isometric force following eccentric and concentric exercise of the elbow flexors. Eur J Appl Physiol. 2006;96(3):235-40. 26. Park R-J, Hwang YT, Park SH. The analysis of knee angular repositioning on knee point position sense in fatigued education. Journal of Special Education & Rehabilitation Science. 2006;45(4):169-90.
27. Changela PK, Selvamani K. A study to evaluate the effect of fatigue on knee joint proprioception and balance in healthy individuals. Medicina Sportiva: Journal of Romanian Sports Medicine Society. 2012;8(2):1851-7.
28. Evans RK, Knight KL, Draper DO, Parcell AC. Effects of warm-up before eccentric exercise on indirect markers of muscle damage. Med Sci Sports Exerc. 2002;34(12):1892-9. 29. Kilduff LP, West DJ, Williams N, Cook CJ. The influence of passive heat maintenance on lower body power output and repeated sprint performance in professional rugby league players. J Sci Med Sport. 2013;16(5):482-6. 30. Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, et al. Physical activity and public health: updated recommendation for adults from the american college of sports medicine and the american heart association. Circulation. 2007;116(9):1081. 33. SENIAM (Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles). Sensor Locations. [cited 2021 April 22];
http://seniam.org/. 34. SENIAM (Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles). Preparation of the skin. [cited 2021 April 22];
http://seniam.org/. 35. Hwang S, Mun MH. Relationship of neck disability index, shoulder pain and disability index, and visual analogue scale in individuals with chronic neck pain. Phys Ther Rehabil Sci. 2013;2(2):111-4. 36. Wagner DR, Tatsugawa K, Parker D, Young TA. Reliability and utility of a visual analog scale for the assessment of acute mountain sickness. High Alt Med Biol. 2007;8(1):27-31. 37. Kim NI, Kim SJ, Jang JH, Shin WS, Eum HJ, et al. Changes in fatigue recovery and muscle damage enzymes after deep-sea water thalassotherapy. Appl Sci. 2020;10(23):8383. 38. Nosaka K, Clarkson PM. Influence of previous concentric exercise on eccentric exercise-induced muscle damage. J Sports Sci. 1997;15(5):477-83. 40. Ostrowski J, Herb CC, Scifers J, Gonzalez T, Jennings A, et al. Comparison of muscle temperature increases produced by moist hot pack and thermostim probe. J Sport Rehabil. 2019;28(5):459-63. 41. Kwon TW, Kim DJ. The effects of warming up intensity and time in strength, muscle power, muscle endurance. Journal of Sport and Leisure Studies. 2007;0(31):853-62. 42. Law RY, Herbert RD. Warm-up reduces delayed-onset muscle soreness but cool-down does not: a randomised controlled trial. Aust J Physiother. 2007;53(2):91-5. 43. Duck-Won O. Effects of Warm-up and Cool-down Exercises for preventing delayed onset muscle soreness on pain and muscle activation. Phys Ther Korea. 2013;20(1):28-35. 44. High DM, Howley ET, Franks BD. The effects of static stretching and warm-up on prevention of delayed-onset muscle soreness. Res Q Exerc Sport. 1989;60(4):357-61. 45. Hiruma E, Uchida M, Sasaki H, Umimura M. Heat pack treatment does not attenuate repeated muscle damage in collegiate females. MedicalExpress. 2015;2(6). 46. Mayer JM, Mooney V, Matheson LN, Erasala GN, Verna JL, et al. Continuous low-level heat wrap therapy for the prevention and early phase treatment of delayed-onset muscle soreness of the low back: a randomized controlled trial. Arch Phys Med Rehabil. 2006;87(10):1310-7. 47. Song QJ, Li YJ, Deng HW. Early and delayed cardioprotection by heat stress is mediated by calcitonin gene-related peptide. Naunyn Schmiedebergs Arch Pharmacol. 1999;359(6):477-83. 48. Lewis SE, Holmes PS, Woby SR, Hindle J, Fowler NE. Short-term effect of superficial heat treatment on paraspinal muscle activity, stature recovery, and psychological factors in patients with chronic low back pain. Arch Phys Med Rehabil. 2012;93(2):367-72. 49. Çakar Hİ, Kara S, Toker O. A wireless surface electromyography system design for lumbar disc herniated patients. 2011 IEEE International Symposium on Medical Measurements and Applications. 2011;IEEE (pp. 35-8).
50. Pereira WM, Ferreira LAB, Rossi LP, Kerpers II, St LACG, et al. Influence of heat on fatigue and electromyographic activity of the biceps brachii muscle. J Bodyw Mov Ther. 2011;15(4):478-84. 51. Kim SH. The Effect of paraffin treatment with exercise on muscle strength and fatigue of the hand according to the use of smartphone. J Korean Phys Ther. 2020;32(4):198-202. 52. Okada K, Yamaguchi T, Minowa K, Inoue N. The influence of hot pack therapy on the blood flow in masseter muscles. J Oral Rehabil. 2005;32(7):480-6. 53. Christie A, Inglis JG, Kamen G, Gabriel DA. Relationships between surface EMG variables and motor unit firing rates. Eur J Appl Physiol. 2009;107(2):177-85. 54. Rodrigues BM, Dantas E, de Salles BF, Miranda H, Koch AJ, et al. Creatine kinase and lactate dehydrogenase responses after upper-body resistance exercise with different rest intervals. J Strength Cond Res. 2010;24(6):1657-62. 55. Machado M, Koch AJ, Willardson JM, Pereira LS, Cardoso MI, et al. Effect of varying rest intervals between sets of assistance exercises on creatine kinase and lactate dehydrogenase responses. J Strength Cond Res. 2011;25(5):1339-45. 56. Felismino AS, Costa EC, Aoki MS, Ferraresi C, Lemos TMdAM, et al. Effect of low-level laser therapy (808 nm) on markers of muscle damage: a randomized double-blind placebo-controlled trial. Lasers Med Sci. 2014;29(3):933-8.
|
|