The Effects of Habitual Aquatic Walking on Arterial Stiffness and Body Composition in Postmenopausal Women: A Cross‑Sectional Study
Article information

Abstract
PURPOSE
Menopause is associated with increased carotid–femoral pulse wave velocity (cfPWV), an indicator of arterial stiffness, which is an independent marker of cardiovascular risk. This study aimed to investigate the cfPWV, blood pressure, and body composition with habitual exercise for at least 1 year in postmenopausal women performing habitual aquatic walking versus age-matched sedentary postmenopausal and premenopausal women.
METHODS
A total of 115 postmenopausal and premenopausal women were divided into the following groups: (1) postmenopausal women performing habitual aquatic walking (HAW; n=57), (2) sedentary postmenopausal women (SPO; n=41), and (3) sedentary premenopausal women (SPR, n=17). The HAW group participated 3 days per week, 60 minutes per day, for at least 1 year, whereas the SPO and SPR groups performed no regular exercise, for less than 2 days per week, 30 minutes per day, for at least 1 year. The cfPWV, BP, and body composition were assessed in all groups.
RESULTS
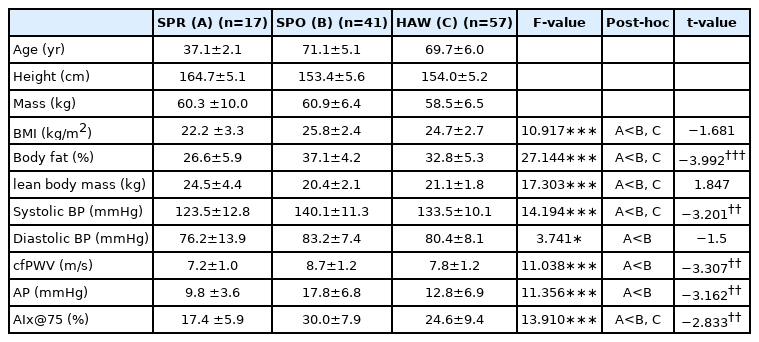
The cfPWV (p<.05), augmentation pressure (p<.05), and DBP were significantly lower in the SPR group than in the SPO group. AIx@75, BMI, %BF, and SBP were significantly lower in the SPR group than in the SPO and HAW groups. Lean body mass was higher in the SPR group than in the SPO and HAW groups (p<.05). The cfPWV, AP, AIx@75, SBP, and %BF were lower in the HAW group than in the SPO group (p<.05). Furthermore, the cfPWV was significantly correlated with aging and SBP.
CONCLUSIONS
This cross-sectional study indicates that sedentary postmenopausal women may be at a higher risk of cardiovascular disease than postmenopausal women who participate in habitual aquatic walking.
INTRODUCTION
Aging is a major risk factor for cardiovascular disease (CVD), and a sedentary lifestyle in older adulthood increases the incidence of CVD in this population [1,2]. Menopause is a natural aging process and is associated with an increased risk of vascular dysfunction and developing CVD. Furthermore, it increases arterial stiffness due to reduced estrogen and elastin levels [3]. CVD is the second leading cause of death in Korean women aged 65 years or older [4]. CVD is caused by a variety of factors, but one of the key contributors is increased arterial stiffness [5]. The main methods to measure arterial stiffness are pulse wave velocity (PWV) and the augmentation index (AI) [6]. Zaydun et al. [7] reported that the incidence of arterial stiffness is higher in postmenopausal women. Increased arterial stiffness reduces baroreflex sensitivity, which in turn has an adverse impact on blood pressure (BP) regulation [8]. The consequent increase in systolic BP leads to increased pulse pressure and left ventricular loading, which elevates the risk of CVD [9].
Regular exercise has been reported to improve microcirculatory vascular function that is responsible for reduced cardiovascular risk in postmenopausal women [10]. Aquatic exercise is a whole-body exercise that utilizes the principle of buoyancy, and it is an ideal exercise for older adults with weakened joints [11]. We have previously shown that aquatic walking exercise for four 60 min utes sessions per week for 12 weeks is effective in improving ambulation in patients with peripheral artery disease [12]. This improvement was determined by important metrics, including leg PWV and BP. In addition, a previous study reported that after a single session aquatic exercise, older women with hypertension had reduced systolic BP (SBP) and diastolic BP (DBP) [13].
While the positive outcomes of aquatic and other exercise regimens have been well documented, no cross-sectional study has investigated the effects of regular exercise and sedentary lifestyle on arterial stiffness, BP, and body composition of postmenopausal women. The aim of this study was to examine these physiological parameters in postmenopausal women who performed habitual aquatic walking exercises for at least 1 year in comparison to a sedentary lifestyle of age-matched participants. We hypothesized that the habitual aquatic walking participants would exhibit decreased arterial stiffness and BP as well as a healthier body composition, compared to the sedentary lifestyle participants.
METHODS
1. Participants
Participants were recruited using flyers from churches and multiple sports centers in South Korea. In this cross-sectional study, a total of 115 women comprised the following groups: 1) habitual aquatic walking postmenopausal women group (HAW; n=57), 2) sedentary postmenopausal women group (SPO; n=41), and 3) sedentary premenopausal women group (SPR, n=17) (Table 1). The HAW group were recruited from multiple sports centers and exercised 3 days per week, 60 minutes per day for at least 1 year. The SPO and SPR groups were recruited from churches and did not exercise regularly (i.e., exercised less than 2 days per week, 30 min utes per day in the previous year). All participants provided written informed consent before their inclusion in the study.
Participant characteristics
2. Body composition
Height (to the nearest 0.1 cm) was measured using a stadiometer (DS102, Jenix, Korea). Body composition was measured using bioelectrical impedance analysis (BIA) (InBody 720, Biospace, Korea), and comprised assessment of body mass (to the nearest 0.1 kg), percentage body fat (%BF; to the nearest 0.1%), and lean body mass (to the nearest 0.1 kg). Body mass index (BMI) was calculated as follows: BMI=body mass (kg)/ height (m2).
3. Blood pressure
All measurements were performed in a noise-free laboratory (25±1°C) in the morning (9:00-11:00 AM). Resting SBP and DBP were measured using an automated sphygmomanometer (BP-203RVIII; Matsunaga Sokki Co., Ltd., Japan) in the seated position after a 5-min ute rest period. The average of two BP measurements was recorded as the resting BP. Resting BP measurements were obtained in accordance with JNC-7 guidelines [14]. The sphygmomanometer cuff was fastened on the right arm, with the lower cuff margin approximately 2 cm above the elbow crease and the arrow on the cuff aligned with the brachial artery.
4. Carotid-femoral pulse wave velocity (cfPWV)
cfPWV was measured using a thigh cuff, carotid tonometry, and a commercially available applanation tonometer (SphygmoCor, AtCor Medical Ltd., Australia) pre-installed with analysis software (version 8.0, SphygmoCor Cardiovascular Management Suite). cfPWV was calculated as the distance between the manubrium sternum to the femoral artery minus the distance between the carotid artery and the manubrium sternum divided by the CF time interval. PWV was calculated using the following formula: PWV=L (distance)/Δ t (time) (m/s) [15].
5. Augmentation pressure (AP), and augmentation index at heart rate (HR) 75 (AIx@75)
Augmentation pressure (AP) was defined as the difference between the second and first systolic peaks. AIx was measured as the augmentation pressure expressed as a percentage of aortic pulse pressure (calculated directly using Pulse Wave Analysis software). AIx was calculated using the following formula: AIx=100×((P2-P1)/(Pulse Pressure)). AIx was normalized to a heart rate of 75 beats/minutes (AIx@75) because it is influenced by heart rate. Two measurements, acquired at 10-second intervals, were averaged [16].
6. Statistical analysis
All data are presented as mean±standard deviation. Statistical analyses were performed with one-way ANOVA with least significant differences post-hoc analyses used to determine differences between specific groups by SPSS 25.0 version software (SPSS Science, Chicago, IL, USA) analysis. Pearson correlation was used to correlate aging and arterial stiffness, and SBP and arterial stiffness. Data (mean±SD) was considered statistically significant at a value of p <.05.
RESULTS
cfPWV was lower in the SPR group than in the SPO group (p<.001), while cfPWV in the HAW group was lower than that in the SPO group (p<.01).
AP was lower in the SPR group than in the SPO group (p <.001), while AP in the HAW group was lower than that in the SPO group (p <.01). AIx@75 was lower in the SPR group than in the SPO and HAW groups (p <.001), while AIx@75 in the HAW group was lower than that in the SPO group (p <.01).
SBP was lower in the SPR group than in the SPO and HAW groups (p <.001), while SBP in the HAW group was lower than that in the SPO group (p <.01). DBP was lower in the SPR group than in the SPO group (p<.05).
BMI was lower in the SPR group than in the SPO and HAW groups (p <.001). %BF was lower in the SPR group than in the SPO and HAW groups (p <.001), while %BF in the HAW group was lower than that in the SPO group (p <.001). LBM was higher in the SPR group than in the SPO and HAW groups (p <.001).
We observed that cfPWV correlated with age (r=0.57, p<.01) and SBP (r=0.52, p <.01) (Figs. 1, 2).
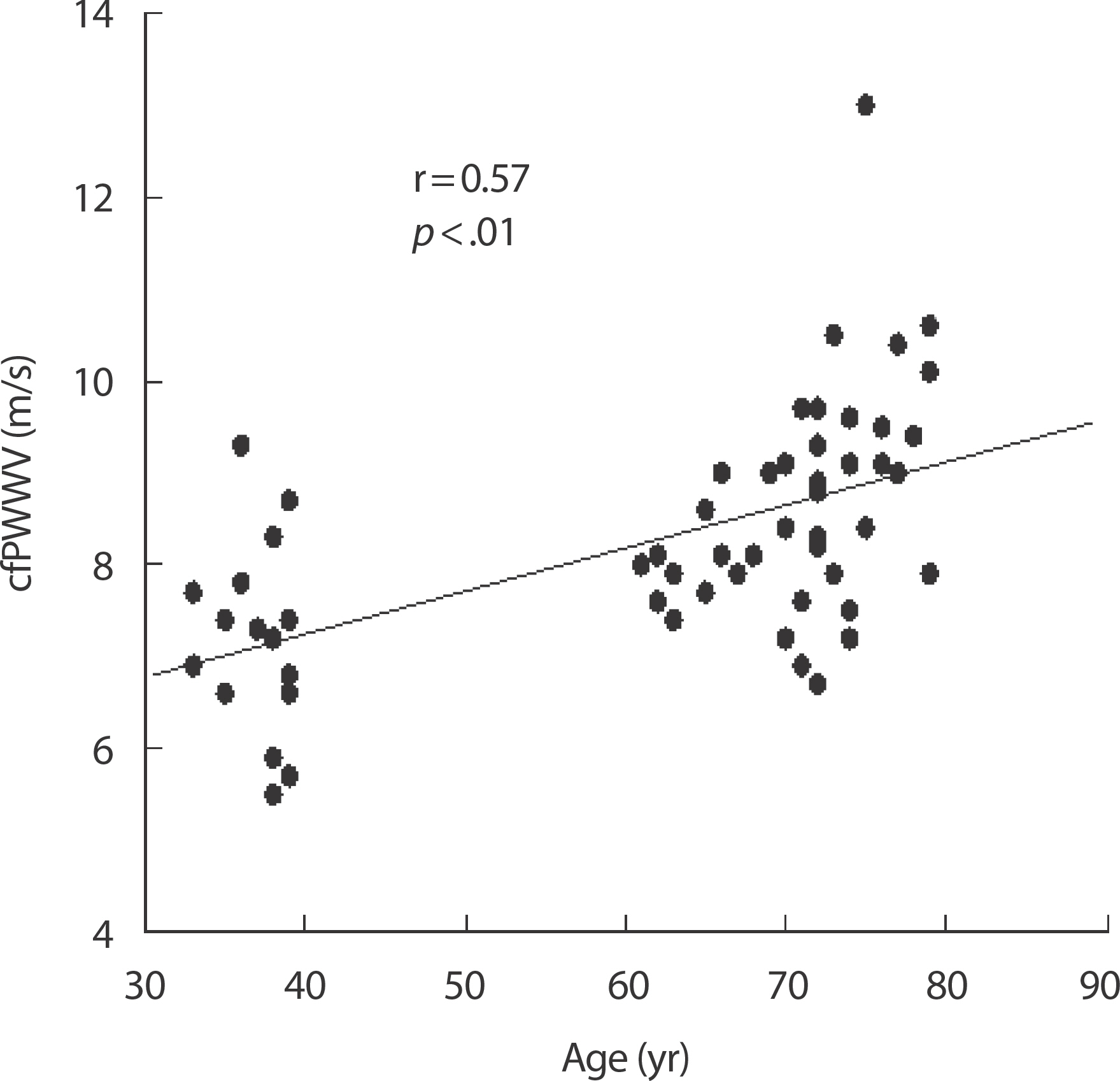
Correlation of cfPWV and age.
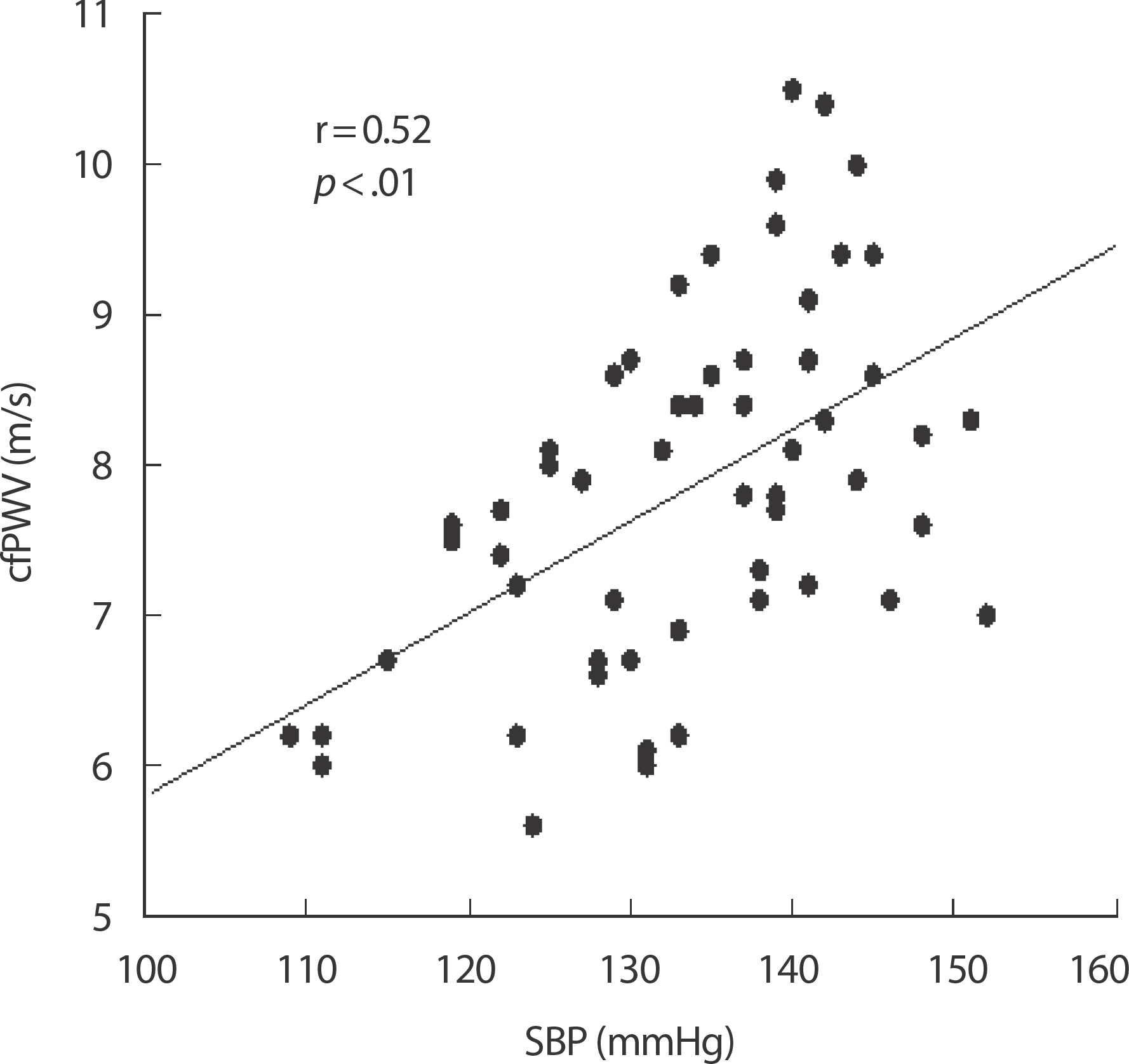
Correlation of cfPWV and SBP.
DISCUSSION
1. Arterial stiffness
Menopause with aging is a major cause of increased arterial stiffness [7]. Aging causes structural changes in the arterial wall that reduces the vasodilation capacity and increases blood flow velocity [17]. In particu-lar, menopause is known to reduce elastin and estrogen concentrations, thereby accelerating arterial stiffness [18]. Previous studies have demonstrated an increase in arterial stiffness and AIx in postmenopausal women [19].
However, exercise is known to improve the risk factors for cardiovascular disease, and previous studies have suggested that cardiovascular functions can be improved in older adults by promoting cardiovascular adaptation through regular aerobic exercise [20]. Matsubara et al. [21] showed that an aerobic exercise program decreased arterial stiffness in menopausal women. One potential mechanism underlying exercise-induced reduction in arterial stiffness is known to involve increased endo-vascular shear stress experienced by blood vessel walls during exercise [22]. Shear stress leads to increased secretion and bioavailability of nitric oxide (NO), a vasodilator, which subsequently improves vascular endothelial cell function and reduces vascular resistance and tone [23]. Additionally, a previous study suggested that a decreased BP is associated with improved arterial stiffness [24]. In the present study, the HAW group showed lower cfPWV, AP, and AIx@75 than the SPO group, and there was a correlation of cfPWV with age and BP. Our results support that notion that arterial stiffness increases due to menopause with aging, and that regular aquatic walking exercise for 1 year or longer may improve arterial stiffness in these women. However, we did not directly examine the vasodilation markers and endothelial function in response to an exercise program. Therefore, further studies evaluating the vasodilation markers and endothelial function are warranted.
2. Blood pressure
Menopause is a known high-risk factor for CVD and is associated with estrogen deficiency in postmenopausal women, causing vascular dysfunction, eventually resulting in increased BP [18]. A previous study reported that increased SBP contributes to CVD risk in older adults [25].
However, another study reported that reduced SBP decreased CVD-associated mortality in middle-aged and older adults [26]. Aerobic exercise is known to improve BP [27], and Forcier et al. [28], in their meta-analysis of 33 studies, demonstrated that individuals who perform high aerobic fitness had significantly reduced SBP and DBP. Furthermore, Arca et al. [29] documented that aquatic walking exercise decreased BP in menopausal women with hypertension.
Reduction in SBP and DBP by regular aerobic exercise, including reduced vascular resistance and vascular tone in the peripheral arteries by improved endothelial function, may be a potential mechanism [30]. Another known mechanism is decreased sympathetic drive due to the reduction of α- and β-adrenergic receptors of sympathetic neurotransmit-ters [31]. This cross-sectional study showed that the HAW group had lower BP than the SPO group. Our findings indicate that habitual aquatic walking exercise can play a significant role in reducing BP in postmenopausal women. However, the mechanism underlying this reduction in BP was not examined in this study. Therefore, future studies should explore the mechanism involved.
3. Body composition
Menopause is associated with a decrease in physiological and metabolic functions, weakening of skeletal muscles, and increase in fat mass [32]. In particular, a reduction of estrogen in postmenopausal women is associated with an increase in their subcutaneous fat mass and abdominal obesity [33]. Notably, abdominal obesity elevates the risk of insulin resistance and arteriosclerosis, and it directly impacts the prevalence of CVD [34,35]. Increased abdominal obesity in menopause is more evi-dent among women than similar-aged men [36]. Therefore, increased abdominal obesity is a prominent concern for the health of older women. However, regular physical activity is considered as the most effective treatment for obesity in older adults [37], and has been shown to mitigate obesity-related metabolic disorders by decreasing body weight [38] and body fat, thereby facilitating metabolic functions by increasing lean mass [39]. Lambert et al. [40] previously demonstrated that aquatic treadmill exercise reduced body weight and %BF in adult men and women, and Bergamin et al. [41] substantiated that aquatic walking exercise improved body composition in older men and women. In the present study, the HAW group showed a lower %BF than the SPO group. We confirmed that regular participation in aquatic walking exercises for 1 year or longer decreased %BF. Therefore, regular exercise may contribute to the effective treatment of obesity in older adults.
CONCLUSION
The results of this cross-sectional study showed that menopause with aging is associated with increased cfPWV, AIx@75, and BP and that regular aquatic walking exercises are linked to improvements in arterial stiffness and BP in postmenopausal women. However, we did not directly examine the vasodilation markers and the mechanism underlying BP reduction due to aquatic exercise programs. Additionally, we did not examine other potential factors that affected arterial stiffness and BP (e.g., daily physical activity level, nutritional intake, etc.). Therefore, future studies should investigate the potential mechanisms underlying Exercise-induced vasodilation and BP reduction, as well as ascertain the influence of other potential factors.
Notes
No potential conflict of interest relevant to this article.
AUTHOR CONTRIBUTION
Conceptualization: WM Son; Data curation: WM Son; Formal analysis: WM Son, JJ Park; Funding acquisition: WM Son, JJ Park; Methodology: WM Son, JJ Park; Project administration: WM Son, JJ Park; Visual-ization: WM Son, JJ Park; Writing-original draft: WM Son, JJ Park; Writing review & editing: WM Son, JJ Park.