규칙적인 유산소 운동 중재가 뇌혈류 감소에 따른 경도인지장애에 미치는 영향
Effects of Regular Aerobic Exercise Interventions on Decreased Cerebral Blood Flow-Induced Mild Cognitive Impairment
Article information

Trans Abstract
PURPOSE
Decreased cerebral blood flow (CBF) is a common symptom in older adults with mild cognitive impairment (MCI). Aerobic exercise is a promising therapeutic intervention for delaying or ameliorating age-related CBF deterioration in older individuals. The review outlines the differences in CBF between healthy older individuals and those with MCI, as well as the benefits of aerobic exercise in augmenting CBF in older adults.
METHODS
We used academic search engines, including PubMed, Web of Science, Scopus, Google Scholar, and the Wiley Online Library, to identify studies demonstrating alterations in CBF with aging and the preventive and therapeutic effects of aerobic exercise on CBF in older adults. The keywords included ‘mild cognitive impairment,’ ‘elderly or older people,’ ‘cerebral blood flow,’ ‘cerebral perfusion,’ and ‘aerobic exercise.’
RESULTS
Aerobic exercise improves or maintains health by enhancing CBF and cognitive function in healthy older individuals. The beneficial impact applies to older people with MCI, although research has been inconsistent regarding aerobic exercise-induced alterations in CBF.
CONCLUSIONS
Aerobic exercise is a promising treatment for MCI in older adults and promotes CBF and cognitive function. However, some studies have reported inconsistent findings regarding changes in CBF. The inconsistencies may be due to several factors, including health and age. Further investigations are warranted to delineate the effects of aerobic exercise on CBF in older adults with MCI.
서 론
오늘날 의학과 과학기술의 발전으로 노인의 기대수명은 증가하였으며, 지금까지의 추이를 고려하면 향후 기대수명은 더욱 높아질 것으로 예상된다[1]. 우리나라는 2000년 고령화 사회로 진입한 이후 노인 인구는 급격히 증가하였으며, 2018년 고령사회를 지나 2025년 65세 이상 노인 인구의 비율이 20.6%을 넘어 초고령사회에 진입할 것으로 보고되고 있다[2]. 초고령사회에 도달하는데 미국은 15년, 일본은 10년이 소요되었지만, 우리나라는 7년으로 경제협력개발기구(Organization for Economic Cooperation and Development, OECD) 국가 중 가장 빠른 추세를 보인다[2]. 노인 인구 증가와 함께 노인 의료비 증가는 불가피하며, 2021년 노인 의료비는 41조 3,829억 원으로 2017년에 비해 1.5배 증가한 것으로 나타났다[3]. 노인성 질환 중 노화와 매우 밀접한 관련이 있는 치매(dementia) 환자 수는 2021년 약 88만 명으로 확인되었으며, 2026년 약 112만 명, 2050년에는 약 300만 명으로 증가할 것으로 예상하고 있다[4]. 또한, 2020년 국가가 부담한 치매 관리비용은 약 17.3조 원이었으며, 이는 2040년까지 56.9조 원으로 증가할 것으로 예상된다[5]. 이는 치매 노인과 부양가족에 대한 경제적-사회적 부담이 나날이 높아지고 있음을 뜻하며, 개인을 넘어 국가 차원에서 치매 예방 및 개선을 위한 시급한 대책 마련이 필요함을 알 수 있다.
경도인지장애(mild cognitive impairment, MCI)는 치매와 달리 일상생활 수행에는 문제가 없지만 기억 장애 등이 있는 경우를 의미한다[6]. 정상적인 인지기능을 가진 노인의 치매 발병률이 1-2%지만, MCI가 있는 노인의 10-15%는 치매로 진전되며, MCI 노인을 대상으로 6년 간 추적 관찰한 결과 대상자의 80%가 치매로 진행됨을 확인하였다[7,8]. 따라서, MCI는 치매로 진행되는 과도기 단계의 질환에 해당하며, 이는 치매로 쉽게 발전하므로 적절한 중재(interventions)를 통한 예방과 악화를 지연하는 것은 매우 중요하다고 할 수 있다[9,10].
뇌혈류(cerebral blood flow, CBF)는 노화가 진행됨에 따라 감소하며, CBF의 감소는 인지기능 저하와 밀접한 관계가 있다[11,12]. MCI는 치매 종류 중 하나인 알츠하이머 질환(Alzheimer's disease, AD)으로 진행되며, 알츠하이머 질환자의 80%가 혈관 병리적 질환(vascular patho-logical complications)을 가지고 있는 것으로 나타났다[13,14]. 이와 더불어, 알츠하이머의 병태생리적 기전(pathophysiological mechanisms) 중 하나로 뇌혈관 기능 이상(cerebral vascular dysfunction)에 따른 CBF 감소를 손꼽을 수 있다[15]. 이에 대한 명확한 기전은 현재 밝혀지지 않았지만 MCI 노인의 심혈관 기능 이상을 살펴보면, 정상 인지기능을 가진 노인보다 MCI 노인은 낮은 CBF를 보이며, 이는 알츠하이머 질환을 초래하는 매개 기전으로 알려져 있다[16,17]. 따라서 MCI 노인의 CBF 를 개선하는 것은 치매를 예방하거나 지연시킬 수 있는 효과적인 방법이라 할 수 있다[18].
규칙적인 운동은 노인기에 경험할 수 있는 낙상, 근감소증, 골다공증, 대사질환, 심혈관 질환 예방에 이바지하며, 개인의 독립적인 일상생활 수행 능력과 삶의 질을 높이는데 일조하는 비약물적 중재 처치(non-pharmacological intervention)이다[19,20]. 다양한 운동 형태 중 유산소 운동은 인지기능뿐 아니라 CBF 및 뇌혈관 기능을 개선하는 방법으로 제시되고 있으며[21], 상반된 연구 결과도 존재하지만 대부분의 연구에서 유산소 운동은 MCI 노인의 인지기능을 개선하는 효과가 있는 것으로 나타났다[22,23]. 따라서 본 종설(review) 연구는 정상 인지기능 노인과 MCI 노인의 CBF 및 뇌혈관 기능의 차이와 이와 관련된 생물학적 기전 그리고 유산소 운동 효과를 규명한 선행연구를 요약하였으며, MCI와 운동 관련 연구에서 활용될 수 있는 임상 변인을 살펴보고자 한다.
뇌혈류 자가조절기전(cerebral autoregulation)
인간의 뇌는 체중의 2%에 불과하지만 중추신경계를 관장하는 중요한 기관이며, 2,000억 개 이상의 신경세포 및 비신경세포와 1조 개의 시냅스, 100 km 이상의 신경섬유, 그리고 600 km에 달하는 혈관으로 구성되어 있다[24,25]. 뇌는 해부학적으로 크게 대뇌(cerebrum), 소뇌(cerebellum), 뇌간(brain stem)으로 나눠진다. 대뇌는 두 개의 대뇌 반구(cerebral hemisphere)로 이뤄지고, 회백질(gray matter)과 백질(white matter)로 불리는 외층과 내층으로 구분되며, 피질은 전두엽(frontal lobe), 두정엽(parietal lobe), 측두엽(temporal lobe), 후두엽(occipital lobe)으로 구성된다. 이렇게 구분된 영역은 기능적으로 상호작용하여 기억, 움직임, 감정, 언어 구사, 학습 및 판단과 같은 모든 인지기능 수행 등을 가능하게 한다[26,27]. 뇌는 신경 활동 과정에서 세포막 사이 이온 경사(ion gradient)와 활동 전위 및 신경 전달의 항상성을 유지하기 위해 많은 양의 에너지를 요구하게 되는데 그 결과 전체 심박출량(cardiac output)의 15%에 해당하는 혈액을 뇌로 보내며, 체내 전체 산소와 탄수화물의 20%와 25%를 각각 소모하게 된다[28,29]. 이는 신체 모든 기관 중 가장 많은 에너지 소모에 해당하나 근육과 달리 뇌는 포도당을 저장하는 능력이 없으므로 혈류를 통한 지속적인 공급에 의존한다는 점에서 CBF의 항상성 유지는 매우 중요하다[30,31].
해부학적으로 좌심실에서 분출된 혈액 중 뇌로 향하는 혈액은 내경동맥(internal carotid arteries, ICA)과 척추동맥(vertebral arteries, VA)을 거쳐 뇌 기저부에서 윌리스환(Circle of Willis)으로 합쳐진다[32]. 이후 뇌의 혈액 공급은 전방 순환과 후방 순환으로 나뉘게 되는데, 전방 순환은 내경동맥에서 나뉘는 전대뇌동맥(anterior cerebral artery, ACA), 중대뇌동맥(middle cerebral artery, MCA)을 통해 전두엽, 측두엽, 두정엽 및 대뇌 반구 대부분의 영역에 혈액을 공급하며, 후방 순환에서는 척추동맥, 기저동맥(basal artery, BA), 후대뇌동맥(posterior cerebral artery, PCA)을 통해 뇌간(brainstem), 소뇌(cerebellum), 후두엽, 내측두엽(medial temporal lobe), 시상(thalamus) 등에 혈액을 공급한다[33,34]. 이러한 과정에서 윌리스환으로부터 유래하는 두개내 동맥(intercerebral arteries)과 연막분지(pial arteries)의 여러 동맥과 세동맥은 뇌 조직을 향해 수직으로 관통하여 내부에서 모세혈관 네트워크(network of capillaries)를 형성하게 되는데, 뇌 조직 내 가스 및 영양소 교환 등은 모두 모세혈관 네트워크인 미세 순환에서 일어난다[25,35].
순환 과정(circulation)에서 원활하게 혈액을 밀어주기 위한 구동력으로서 뇌관류압(cerebral perfusion pressure)이 작용한다. 뇌혈관 내 압력(cerebral intravascular pressure)은 일정한 범위 내에서 변동(fluctuation)이 있더라도 CBF를 일정하게 유지하기 위하여 호르몬 및 신경 전달 물질과 관계없이 뇌혈관은 수축 또는 이완하게 되는데 이를 뇌혈관 자동조절(cerebral autoregulation)이라 한다[36]. 평균 뇌관류압은 60-80 mmHg이고 평균 동맥압은 70-100 mmHg를 형성하고 있으며, 뇌관류압 또는 평균 동맥압 증가는 일시적으로 혈류량을 증가시키지만 뇌혈관 자동조절 기전에 의해 혈관이 수축됨으로써 혈관 저항을 높여 혈류량을 감소시킨다. 반대로, 뇌관류압 또는 평균 동맥압이 감소할 경우 혈액 순환에 필요한 구동력을 잃게 되어 혈류량은 감소하게 되는데 이를 보완하기 위해 혈관 이완을 통한 혈관 저항을 낮춤으로써 혈류량을 증가시키게 된다[37]. 이러한 뇌혈관의 자동조절 기전을 통해 정상 혈압을 가진 성인의 경우 CBF는 분당 뇌 조직 100 g당 약 50 ml로 유지되며, 자동조절 기능은 뇌혈관에서 특히 발달된 것으로 알려져 있다[38]. 이상에서 기술한 기전은 근원성 기전(myogenic mechanism)에 해당하며, 자동조절 기전 외에도 뇌혈류량 조절에 관여하는 기전으로 신경성 기전(neurogenic mechanism), 대사성 기전 (metabolic mechanism), 그리고 혈관내피성 기전(endothelial mechanism)을 들 수 있다.
근원성 기전 혹은 근원성 반응(myogenic response)은 혈관 내 압력 변화에 반응하여 혈관 수축과 이완에 관여하는 혈관평활근(vascular smooth muscle cell, VSMC)의 고유 기능에 해당하며, 혈관 내 압력 변화는 기계 감응성 이온 통로(mechanosensitive ion channels) 및 수용체(mechanosensitive receptors)에 의해 감지되며, 이후 하위 기전 활성화로 근원성 반응이 일어난다[39]. 예를 들어, 증가한 혈관 내 압력은 혈관평활근에 분포한 기계 감응성 이온 통로 또는 수용체를 활성화(acti-vation)하며, 이는 양이온(cation)의 유입을 통해 혈관평활근 세포막의 탈분극(pressure-induced VSMC depolarization)을 야기한다[40,41]. 혈관평활근의 탈분극은 전압 의존성 칼슘 통로(voltage-dependent calci-um channels)를 열리게 하며, 이를 통해 혈관평활근 내부로 칼슘 이온이 유입된다[40,41]. 유입된 칼슘 이온은 칼모듈린(calmodulin)과 결합하여 myosin light chain kinase (MLCK)를 활성화하며, 이를 통한 myosin light chain의 인산화(phosphorylation)는 혈관 수축으로 이어지고 혈관 직경을 감소시킴으로써 CBF를 조절하게 된다[42].
각각의 뇌 영역은 에너지를 소비하는 수준이 다르며, 이에 비례하는 수준으로 관류(perfusion)되므로 뇌의 국소적 신경 활동 정도에 따라 CBF의 증가는 달라진다[43]. 기능성 충혈(functional hyperemia) 또는 뇌신경 혈관 연접(neurovascular coupling, NVC)은 신경세포의 대사 활동 증가에 따라 요구되는 에너지를 충족하기 위해 CBF를 증가시키는 역할을 담당한다[44]. 혈관평활근, 신경세포(neurons), 성상교세포(astrocytes), 뇌혈관장벽(blood-brain barrier, BBB) 및 주피세포(pericytes) 등은 서로 어우러져 신경-혈관 단위(neurovascular unit)를 형성하며, 세포 간 상호작용을 통해 국소적인 혈류 변화를 유도하는데 신경세포, 성상교세포, 미세 아교세포(microglia) 등은 혈관 확장 물질(예: 아세틸콜린(acetylcholine), 산화질소(nitric oxide)) 또는 혈관 수축 물질(예: 세로토닌(serotonin), 신경 펩타이드 Y (neuropeptide Y, NPY))을 분비하여 혈관 직경을 조절한다[45-47].
대사성 기전은 주로 미세혈관(microvasculature)의 직경 조절에 영향을 미치며, 특히 동맥혈 이산화탄소 분압(partial pressure of arterial carbon dioxide, PaCO2)에 의해 혈관 직경이 조절된다[37]. PaCO2는 혈관 조절에 큰 영향을 미치며, PaCO2가 1 mmHg 증가할 때마다 CBF는 4% 정도 증가하는 것으로 알려져 있다[48]. 따라서 과탄산혈증(hyper-capnia)과 같이 PaCO2가 과도하게 증가한 경우 뇌혈관은 확장되어 CBF는 증가하며, 이와 반대로 저탄산혈증(hypocapnia, PaCO2 저하)은 혈관 수축을 통해 CBF를 감소시키는 것으로 보고되었다[49]. 이외에도 동맥혈 산소 분압(partial pressure of arterial oxygen, PaO2)과 혈중 글루코스 농도 역시 CBF 조절 인자에 해당하며, PaO2가 50 mmHg 이하로 떨어질 경우 혈관 확장으로 인한 CBF 증가가 나타나고 2 mmol/L 이하의 저혈당 상태에서도 유사한 혈관 반응이 나타난다[39],
뇌혈관의 혈관내피세포(endothelial cell, EC)는 혈액과 혈관 사이의 장벽 역할을 할 뿐만 아니라 내분비 기관으로서 다양한 물질들을 합성하고 분비하며, 혈관 긴장(vascular tone), 혈관 투과성(vascular permeability), 국소 염증반응(local inflammatory response) 등을 매개하는 역할을 담당한다[50,51]. 뇌혈관의 혈관내피세포는 혈류에 의한 전단응력(shear stress)과 혈압 등의 물리적 자극에 직접 노출되며, 혈관평활근 및 혈관 주변의 신경세포와 생물학적 신호를 주고받으며 혈관 조절에 관여한다[40]. 혈관내피세포는 MEPs (myoendothelial projections)라는 특수한 구조물(혈관내피세포의 돌출된 부분으로 internal elastic lamina fenestrae를 지나 혈관평활근 세포와 신호 전달이 가능함)을 통해 혈관평활근과 인접해 있으며, MEGJs (myoendothelial gap Junctions)를 통해 두 세포(혈관내피세포-혈관평활근) 간에 다양한 화학적-전기적 신호를 교환할 수 있다(chemical or electrical intracellular communication). 예를 들어, 혈관내피세포에서 활성화된 이온 통로에 의해 일어난 세포막의 과분극(hyperpolarization)은 MEGJs를 통해 혈관평활근으로 전달되어 전압 의존성 칼슘 통로를 폐쇄함으로써 칼슘 유입을 차단하여 혈관 확장을 일으키는데 기여한다[40,52,53].
노화에 따른 혈관 기능 및 CBF 감소
노화에 따라 나타나는 기능적 ∙ 대사적 변화는 신경세포의 변화로 이어지며, 퇴행성 신경질환(neurodegenerative diseases)을 초래한다[54]. 노화는 CBF에도 부정적인 영향을 미치는데 일반적으로 CBF는 뇌 조직 100 g에 분당 55 mL의 혈액이 공급되지만[55], 중년 이후 매년 0.38%에서 0.45%까지 CBF는 지속적으로 감소한다[56,57]. 뿐만 아니라 노인들을 대상으로 2년간 CBF 변화를 추적 관찰한 결과 CBF에 직접적인 영향을 미치는 뇌혈관 저항이 증가하는 것을 확인하였으며, 이는 대뇌피질 위축과 부적 상관관계가 있음이 보고되었다[58]. 이러한 맥락에서 노인에게 나타나는 만성적인 CBF 감소와 퇴행성 신경질환은 상당한 관련성이 있으며, 노화에 따른 CBF 감소 기전은 명확히 밝혀지지 않았으나 다양한 요인(예: 노화로 인한 동맥의 탄력저하, 뇌신경 세포의 염증 반응, 대뇌 조직의 아밀로이드 침착 등)이 복합적으로 작용한 결과로 사료된다[59].
기능성 충혈(functional hyperemia; 대사적 요구에 따라 혈류량이 증가하는 것을 의미)은 노화에 따라 손상되는 것으로 보고되고 있다. 젊은 성인과 노인에게 인지 과제를 줬을 때 두 집단 모두 전대대동맥과 후대대동맥의 뇌혈류 속도(cerebral blood flow velocity, CBFv)가 증가하였으나, 노인의 경우 후대대동맥의 뇌혈류 속도가 젊은 성인보다 현저하게 낮았다[60,61]. 노화에 의한 기능성 충혈 손상은 연령 증가에 따른 활성산소종(reactive oxygen species, ROS) 증가가 주요 원인이며, 활성산소 증가는 뇌 미세혈관과 신경 세포의 상호작용인 뇌신경 혈관 연접(NVC) 손상을 야기하여 기능성 충혈을 낮추는 것으로 보고되었다. 크산틴 산화효소(xanthine oxidase), 산화질소(nitric oxide) 또는 아라키돈산(arachidonic acid) 대사에 관여하는 효소 등은 뇌 조직의 활성산소 증가를 초래하며[62,63], 노화된 뇌 신경세포의 손상된 미토콘드리아 또한 활성산소 생성의 주된 이유로 보고되었다[64].
뇌와 혈관에서 생성된 활성산소는 니코틴아마이드 아데닌 디뉴클레오타이드 인산 산화효소(nicotinamide adenine dinucleotide phosphate (NADPH) oxidase)에 의해 대부분 생성되며[65], 노화 쥐의 경우 활성산소 중 하나인 과산화물(superoxide, O2-)과 산화질소가 반응하여 과산화질산염(peroxynitrite)을 형성하여 산화질소의 생체이용률(bioavailability)을 감소시켜 혈관내피세포 기능 손상(endothelial dysfunction)을 야기하는 것으로 보고되었다[66]. 특히, 뇌 미세혈관의 활성산소에 의한 혈관내피세포의 산화질소 생성 저하는 기능성 충혈 및 CBF 감소로 이어지며[61], 약물적 중재 처치를 통한 NADPH 산화효소 억제는 노화 쥐의 CBF를 증가시킨 것으로 나타나[67] 활성산소 생성과 산화질소 생체이용률(nitric oxide bioavailability) 감소가 기능성 충혈과 CBF 조절에 큰 영향을 미치는 것을 확인할 수 있다.
노화에 의한 혈관내피세포 기능 이상(aging-induced endothelial dysfunction)은 뇌혈관장벽과 뇌신경 혈관 연접(NVC) 손상과 함께 발생하며, 이와 같은 기능 이상은 대뇌 동맥(cerebral arteries)에서 뇌 조직 내에 분포하는 세동맥(cerebral parenchymal arterioles)에 이르기까지 전반적으로 나타난다[43]. 노화는 혈관내피세포 산화질소 합성효소(endothelial nitric oxide synthase, eNOS) 조절 및 산화질소 생성 억제뿐만 아니라 혈관 신생(angiogenesis) 저하 및 뇌신경 염증반응을 초래하여 뇌신경 혈관 연접과 뇌혈관 기능장애를 일으킨다[68]. 뇌신경 및 혈관 신생에 기여하는 뇌유래신경영양인자(brain-derived neurotrophic factor, BDNF)와 혈관내피성장인자(vascular endothelial growth factor, VEGF) 등은 노화로 감소하며, 세포 노화 관련 분비 표현형(senescence-associated secretory phenotype, SASP) 증가는 신경세포의 염증을 유도하여 혈관내피세포 내 간극 연접(gap junction) 및 뇌혈관장벽 손상을 초래하고 활성산소 증가 및 eNOS/NO 기전에 부정적인 영향을 미쳐 혈관내피세포 기능 이상을 야기하는 것으로 보고되었다[69,70]. 혈관내피세포의 기능 손상은 대뇌 CBF 및 관류(perfusion)를 저하하며, 궁극적으로 신경세포사멸 및 인지기능 장애를 일으킨다. 혈관내피세포의 밀착 연접(tight junction)을 구성하는 단백질(예: claudins, occludins 등)의 변화는 뇌혈관장벽을 손상시켜 투과율(permeability)을 증가시키는 것으로 보고되었으며, 이는 노화뿐만 아니라 뇌혈관 질환에서 관찰되는 증상으로 알려져 있다[69,71,72]. 노화 과정에서 발생하는 IL-6 및 IL-1β와 같은 전염증성(pro-inflammatory) SASP 인자는 신경 염증을 유도하며, 혈관내피세포의 밀착 연접 손상에 따른 ROS 증가와 산화질소 생성 저하는 뇌혈관장벽과 뇌신경 혈관 연접 이상을 초래하는 것으로 보고되었다[69,71,72]. 또한, 노화에 의한 SASP의 증가는 염증성 사이토카인(inflammatory cytokines)을 증가시키며, 이는 혈관 외벽(vascular adventitia)을 구성하는 탄성 단백질(예: 콜라겐(collagen), 엘라스틴(elastin))을 분해하는 matrix metalloproteinase-2 (MMP-2)와 matrix metalloproteinase-9 (MMP-9)을 증가시켜 뇌혈관장벽을 손상시킨다[70,73,74].
노화에 따른 교감신경 과활성(sympathetic hyperactivity), 만성 염증 증가, 산화 스트레스에 의한 고혈압 등은 혈관 리모델링(vascular remodeling)과 뇌혈관 자가조절능력(autoregulation) 손상으로 이어지며, 이는 만성적인 CBF 감소에 결정적인 역할을 하는 것으로 알려져 있다[66,75-77]. 고혈압은 뇌혈관의 구조적 변화를 초래하며, 혈관의 비대화와 같은 리모델링을 통해 혈관 벽 두께(vascular wall thickness)를 증가시킨다[78]. 고혈압을 유발한 동물모델에서 뇌혈관 리모델링이 관찰되었으며, 증가한 혈관 외벽 두께 및 동맥경직도(arterial stiffness)는 CBF 감소에 기여한 것으로 보고되었다[79,80]. LaPlace 법칙(LaPlace's Law)에 따르면, 혈관벽에 가해지는 장력(wall tension)은 내강의 압력과 혈관의 반지름을 곱한 값이며, 혈관벽에 가해지는 스트레스(wall stress)는 혈관벽 두께에 혈관벽에 가해지는 장력을 나눈 값으로 나타낼 수 있다. 고혈압은 혈관벽의 장력과 스트레스 증가로 이어지며, 뇌혈관의 리모델링을 통한 혈관벽 두께의 증가는 CBF의 항상성을 위한 보호 작용 혹은 기능 저하에 따른 보상적인 구조변화로 볼 수 있다[79].
그러나, 대뇌동맥 혹은 뇌 미세혈관의 리모델링은 혈관의 내강 직경과 혈관 확장 능력을 감소시켜 뇌의 저관류(hypoperfusion)와 혈역학적(hemodynamic) 손상을 유발할 뿐만 아니라 비대해진 뇌혈관의 혈관 평활근은 혈압 변화에 따라 혈관 수축과 이완이 결정되는 근원성 반응(myogenic response)의 이상을 초래하여 과도한 혈관 수축에 따른 CBF 감소를 초래한다[81-83]. 엔지오텐신 II (angiotensin II)를 주입하여 고혈압을 유발한 동물모델의 중대뇌동맥(MCA) 혈관평활근에서 근원성 반응에 관여하는 비선택성 양이온 투과 이온 통로(nonselective cationion channel)인 TRPC6 (canonical transient receptor potential 6) 이온 통로 발현(expression)이 증가하였으며, 이를 통한 혈관평활근 탈분극(depolarization) 증가는 과도한 근원성 반응 증가와 함께 CBF 감소를 초래한 것으로 보고되었다[84-87]. 노화가 진행됨에 따라 증가하는 것으로 보고된 엔지오텐신 II는 제1형 엔지오텐신 수용체(angiotensin II receptor type 1, AT1 R)를 통한 혈관 수축 기전[88-90]뿐만 아니라 NADPH 산화효소 활성화를 통한 활성산소 생성에 관여하며[91-93], 이는 혈관 탄성 단백질 분해효소 MMP-9을 자극하여 혈관 리모델링을 유발하는 것으로 알려져 있다[74,94].
알츠하이머 질환 및 경도인지장애 유발 원인으로 잘 알려진 아밀로이드-베타 침착(amyloid-beta aggregation)은 노화에 따라 나타나는 자연스러운 현상이며, 혈관질환을 야기하는 주요 원인에 해당한다[95,96]. 아밀로이드-베타는 NADPH산화효소를 통해 활성산소를 증가시키며, 증가된 활성산소는 강력한 혈관 수축 인자인 엔도세린-1 (endothe-lin 1, ET-1)을 증가시켜 대뇌동맥 및 뇌 미세혈관을 수축시킨다[97,98]. 이를 뒷받침하듯, 경도인지장애 및 알츠하이머 질환 노인을 대상으로 양전자 단층촬영(positron emission tomography, PET)을 실시한 결과 아밀로이드-베타 양성인 노인에서 유의하게 증가한 뇌혈관 저항과 위축된 대뇌피질이 관찰되었다[58].
MCI 노인에게 나타나는 뇌혈류의 변화
혈류 변화에 민감한 뇌 조직은 노화에 따른 CBF 감소로 인해 다양한 질환에 노출된다. 혈관 기능 이상으로 CBF의 과도한 증가는 뇌 조직의 부종(edema) 및 뇌 미세혈관 파열에 따른 뇌출혈(brain hemor-rhage) 등을 초래하며, 만성적인 CBF 감소는 뇌신경 세포의 세포사멸을 야기한다[99-101]. 이와 더불어, 뇌혈관 이완 기능 저하와 CBF의 장기적인 감소는 알츠하이머 질환과 같은 퇴행성 뇌신경 질환을 유발하는 것으로 알려져 있으며, 알츠하이머 질환 전단계에 해당하는 MCI 역시 감소한 CBF에 의한 것으로 많은 선행연구를 통해 밝혀졌다[102-104].
노화의 진행에 따라 평균 뇌혈류 속도(CBFv)는 감소하며, 중대뇌동맥(MCA)과 전대뇌동맥(ACA)에서 뇌혈관 저항을 나타내는 박동 지수(pulsatility index, PI)와 저항 지수(resistance index, RI)가 증가하는 것으로 보고되었다[105]. 연령 증가에 따른 중심 동맥 경직도(central arterial stiffness) 증가는 뇌혈관의 저항을 더욱 높이는 원인 중 하나로 보인다[106]. 또한, MCI 노인의 경우 중대뇌동맥의 휴식 시 박동 지수와 저항 지수가 정상 인지 노인에 비해 현저하게 높았으며, 동맥혈 이산화탄소 분압(PaCO2) 증가에 따른 뇌혈관 직경 조절 능력을 나타내는 지표(breath holding index, BHI) 또한 유의하게 낮은 것으로 보고되었다[107]. 그럴 뿐만 아니라 MCI 노인을 24개월간 추적 조사하여 알츠하이머 질환으로 진행된 연구대상자의 중대뇌동맥을 측정한 결과, 이들은 낮은 BHI와 높은 박동 지수 및 저항 지수를 보였으며, 치매 평가 도구인 간이정신상태검사(mini-mental state examination, MMSE) 점수의 감소와 박동/저항 지수 증가는 높은 연관성이 있는 것으로 확인되었다[108]. 이에 낮은 BHI와 높은 박동/저항 지수는 MCI 판정과 알츠하이머 질환 진행 예측 임상 인자로써 사용되고 있다[109].
전술한 바와 같이, MCI와 알츠하이머 질환은 연령 증가에 따른 CBF 감소와 밀접한 연관성이 있다[110]. 흥미로운 것은 노화에 의한 CBF 감소 패턴은 뇌 영역에 따라 다른 양상을 보인다는 점이다. 다수의 선행연구를 분석한 메타분석 연구에 따르면, 정상 인지기능 노인에 비해 MCI 노인의 경우 측두엽(temporal lobe), 중전두엽(middle frontal lobe), 두정엽(parietal), 하두정엽(inferior parietal), 각회(angular gyrus), 설전부(precuneus), 후방 대상 피질(posterior cingulate cortex, ACC), 시상(thalamus), 기저핵(basal ganglia) 등의 구역(region)에서 안정 시 혈류 저하가 보고되었고[111], 2년 내에 치매로 진전된 MCI 노인의 경우 치매로 진전되지 않은 MCI 노인보다 전두엽, 측두엽, 두정엽, 후두엽에서 감소된 혈류량을 보였으며, 특히 측두엽 영역 중 좌측 내측두엽에서 비정상적인 혈류 감소가 두드러지게 나타났다[112]. 그러나, 일부 연구에서는 MCI 노인의 전두엽, 우측 측두이랑하 영역(temporal sub-gyral regions), 좌측 해마(hippocampus), 우측 편도체(amygdala), 우측 미상핵(caudate nucleus), 복측피각(ventral putamen), 담창구(globus palli-dus)의 CBF가 증가된 것으로 보고된 바 있다[113,114]. 따라서, 신경 퇴행 및 인지기능 저하는 뇌의 특정 영역 국소 뇌혈류(regional cerebral blood flow, rCBF) 증감과 밀접한 관계가 있으며[115], 이러한 혈류 패턴의 변화는 인지기능 저하 및 치매 전단계에서 나타나는 보상 메커니즘으로 제시되고 있다[112,116,117]. 이 기전은 현재 명확하게 규명되지 않았으나 병리적인 신경 활동의 증가, 신경 염증 및 혈관 확장 및 혈관 밀도 변화를 통한 혈액 공급 조절 기전의 변화로 설명된다고 보고되었다[101,118].
유산소 운동이 MCI에 의한 CBF 감소에 미치는 영향
유산소 운동은 노인에게 나타나는 고혈압, 동맥경직도 증가, 혈관내피세포 기능 저하, 이상지질혈증, 제2형 당뇨병 등 혈관질환 위험인자[119-122]와 감소한 CBF 및 인지기능 개선에 효과적인 방법으로 제시되고 있다[123-126]. 또한, MCI 노인에게 유산소 운동은 혈관신생 인자(angiogenesis factors)와 신경영양인자(neurotrophic factors) 등의 증가에 기여하여 뇌 건강에 긍정적인 영향을 미치는 것으로 보고되었다[127-130]. 따라서, 정상 인지 노인뿐 아니라 MCI 노인 또한 유산소 운동을 통해 긍정적인 이점을 얻을 수 있다.
MCI 노인을 대상으로 유산소 운동 프로그램 적용 후 CBF 변화를 중점적으로 관찰한 연구를 정리한 내용이다. Tomoto et al. [131]은 12개월간 건망증을 동반한 경도인지장애(amnestic mild cognitive impairment, aMCI) 노인을 대상으로 유산소 운동 프로그램을 적용하였으며, PaCO2 증감에 따른 뇌혈관 반응도(cerebral vasomotor reactivity)와 인지기능과의 상관관계를 분석하였다. 유산소 운동 중재 처치 후 안정 시 뇌혈류와 관련된 변화는 없었으나 과호흡(hyperventilation)을 유도하였을 때 aMCI 노인의 저탄산혈증에 대한 뇌혈류 속도와 뇌혈관 전도도(cerebrovascular conductance)가 증가하였고, 산소저장백을 이용하여 연구대상자가 같은 공기를 호흡하게 함으로써 유도한 고탄산혈증에 대해서는 뇌혈류 속도와 혈관 전도도가 감소한 것으로 나타났다. 동일 연구에서 유산소 운동 중재 처치 이후 증가한 VO2 peak와 저-고탄산혈증에 대한 뇌혈관반응도(즉 뇌혈류 속도와 혈관 전도도)는 서로 연관성이 있으며, 증가한 인지기능과 감소한 고탄산혈증에 대한 뇌혈관 반응도는 서로 부적상관관계가 있는 것으로 보고했다[131]. 이는 정상 인지기능을 가진 노인을 대상으로 유산소 운동 프로그램을 적용한 결과 과탄산혈증 유발 시 혈류속도가 증가하는 양상과 대비되는 결과이다[132,133]. 이상의 결과를 종합하면 유산소 운동은 대뇌 동맥 경직도를 개선함으로써 뇌혈관 긴장도(cerebral vascular tone)를 낮추며, 대뇌 동맥의 혈관내피세포 기능 개선은 혈중 CO2 농도 증가에 따른 혈관 확장 능력 향상으로 이어짐을 알 수 있다[131]. aMCI 노인을 대상으로 12개월 동안 유산소 운동을 실시한 다른 선행연구에서도 경동맥 경직도, 중심 동맥 경직도, CBF 박동 지수 감소가 확인되었으며, 뇌혈류 속도와 총 CBF가 증가한 것으로 보고되었다[134].
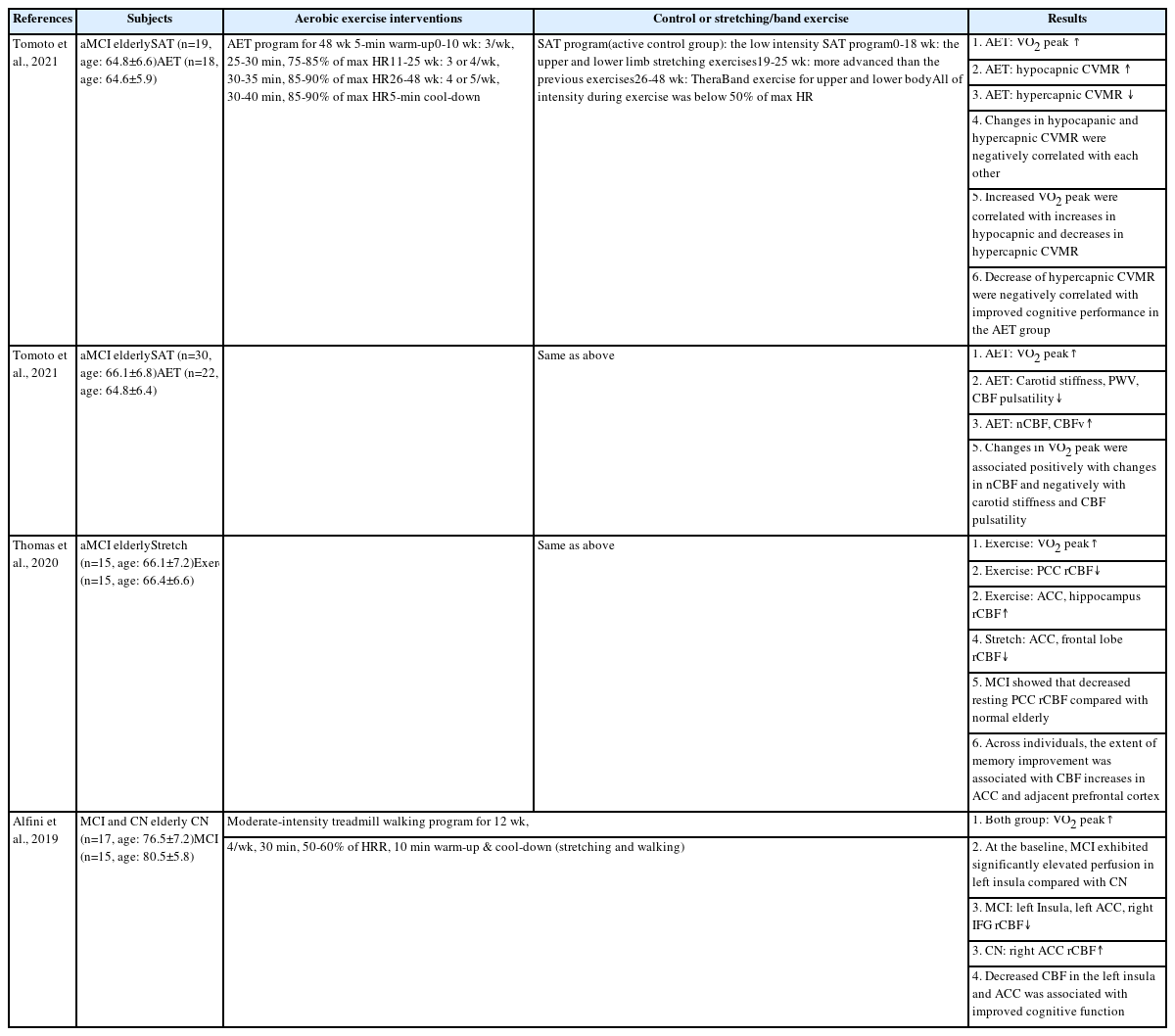
Characteristics of aerobic exercise intervention to MCI
Thomas et al. [135]은 12개월간 aMCI 노인에게 유산소 운동과 스트레칭 운동을 집단별로 적용한 결과, 유산소 운동집단에서 전방 대상 피질(anterior cingulate cortex, ACC)과 해마의 국소 뇌혈류(rCBF)가 증가한 반면, 후방 대상 피질(posterior cingulate cortex, PCC)의 rCBF는 감소하였다. 이와 반대로 스트레칭 운동집단의 경우 전방 대상 피질과 전두엽의 rCBF는 감소하였으나, 전방 대상 피질과 전전두 피질(prefrontal cortex)의 rCBF 증가하였으며, 두 운동 집단의 rCBF 증가는 인지기능의 개선과 깊은 관련이 있는 것으로 보고되었다. 즉 유산소 운동 후 후방에서 전방으로 혈류가 재분배되는 것을 확인하였으며, 전두엽의 CBF 증가는 개선된 기억력과 연관성이 있는 것으로 보인다[135]. 그러나, 후방 대상 피질의 rCBF는 유산소 운동 후 감소하였다. 유산소 운동은 후방 대상 피질의 rCBF 감소 개선에 기여하지 못했지만 이러한 rCBF 패턴의 변화는 유산소 운동 후 전방 대상 피질의 부피 증가 과정에서 나타나는 신경 활동과 유사한 패턴을 보이는 것으로 제시되었다[136]. 한편, Alfini et al. [137]은 12주간 MCI 노인에게 유산소 운동을 적용한 결과 좌측 뇌섬(insular), 전방 대상 피질 및 전두엽에 위치한 우측 하전두회(inferior frontal gyrus)의 rCBF가 감소하였으며, 감소한 전방 대상 피질과 뇌섬의 rCBF는 증가한 인지기능과 상관관계가 있는 것으로 나타났다[135]. 또한, 유산소 운동 참여 이전 MCI 노인에게서 좌측 뇌섬의 증가한 rCBF를 확인하였으나, 운동 중재 이후 정상 노인과 동일한 수준으로 감소한 것으로 보고 되었으며[135], 특히 알츠하이머 위험군에서 보고된 뇌섬의 과관류(hyperperfusion)를 개선시켰다는 점에서 유산소 운동의 긍정적인 효과를 확인할 수 있었다[138]. 본 연구에서 흥미로운 점은 Thomas et al. [135]의 연구에서 제시된 전방 대상 피질의 rCBF의 증가와 상반된 결과를 보였다는 것이며, 이는 두 연구에 참여한 대상자의 연령, MCI가 진행된 기간 혹은 운동 프로그램 요소(예: 운동 강도, 빈도, 시간 등)의 차이에서 기인한 것으로 판단된다. 또한, 연령에 의한 아밀로이드 침착[139] 혹은 Alfini et al. [137] 의 연구에서는 평가되지 않았지만, 노인의 경우 연령이 증가할수록 운동 트레이닝에 의한 해마의 rCBF가 오히려 감소한다는 연구 결과[125]를 바탕으로 연령에 따른 유산소 운동 효과가 다르게 나타날 가능성 또한 배제할 수 없다. 따라서 선행연구에서 확인된 상이한 연구 결과를 검증하기 위해 다양한 운동 프로그램과 MCI 노인을 대상으로 많은 후속 연구가 필요할 것으로 생각한다.
결 론
우리나라는 초고령사회로 급격히 전환되고 있고, 치매 환자의 수는 매년 증가하고 있으며 이에 대한 환자 개인, 부양 가족과 사회의 부담은 나날이 늘어가고 있으므로 이를 해결하는 방안 마련이 절실하다. 노화의 진행과 함께 나타나는 CBF 감소는 경도인지장애 및 알츠하이머 질환의 주요 원인에 해당하며, 이를 예방하고 지연시키는 중재 처치로 유산소 운동을 손꼽을 수 있다. 유산소 운동은 노인의 삶의 질과 독립적인 생활을 영위하는 데 이바지하며, 노화로 인해 감소한 CBF를 개선하는 것으로 알려져 있다. 유산소 운동의 이와 같은 효과는 MCI 노인의 인지기능 개선에 기여한 것으로 대부분의 선행연구에서 규명되었다. 그러나, 몇몇 연구에서는 유산소 운동이 MCI 노인의 CBF와 인지기능 개선에 뚜렷한 효과가 밝혀지지 않았으며, 이는 개인적인 특성(예: MCI 질환 정도, MCI 유발 원인, 만성질환, 생활 습관 등)과 운동 프로그램의 이질성에 기인한 것으로 생각한다. 따라서, 유산소 운동 프로그램의 운동처방적 요소(예: 운동 강도, 빈도, 시간 등)를 다양하게 적용하고, 운동 프로그램이 MCI 노인의 인지 기능 변화에 영향을 미칠 수 있는 가외 변인(extraneous variables)을 통제하여 운동 프로그램의 효과를 검증하는 후속 연구가 필요할 것으로 판단된다. 또한, 뇌혈류량 감소를 초래하는 중심 동맥경직도(central arterial stiffness) 증가와 혈관내피세포 기능이상(endothelial dysfunction)을 효과적으로 개선할 수 있는 유산소 운동 프로그램을 개발하고 관련된 생물학적 기전(biological mechanisms)을 밝히는 것 또한 MCI 개선 및 인지기능 향상에 이바지할 것으로 생각된다.
Notes
이 논문 작성에 있어서 어떠한 조직으로부터 재정을 포함한 일체의 지원을 받지 않았으며, 논문에 영향을 미칠 수 있는 어떠한 관계도 없음을 밝힌다.
AUTHOR CONTRIBUTIONS
Conceptualization: DH Lee, KS Hong; Data curation: DH Lee, SC Sung; Formal analysis: DH Lee, SC Sung, KS Hong; Funding acquisition: KS Hong; Methodology: DH Lee, SC Sung, KS Hong; Project administration: DH Lee, KS Hong; Visualization: DH Lee; Writing - origi-nal draft: DH Lee, KS Hong; Writing-review & editing: DH Lee, SC Sung, KS Hong.