Association of Grip Strength with All-Cause Mortality among Korean Adults with Disabilities
Article information

Abstract
PURPOSE
This study utilized data from the Korean Longitudinal Study of Aging to investigate the association between grip strength and all-cause mortality rates in adults with disabilities aged ≥45 years in Korea.
METHODS
The study included 430 adults with disabilities without missing values in the mortality variable and no history of cancer, cerebrovascular diseases, or cardiovascular diseases (mean age 63.2±10.0 years) for analysis. Data from the first to seventh waves were used in the analysis. Grip strength was measured using a dynamometer, and mortality status and date were recorded. A Cox proportional hazards model was used to examine the association between grip strength and all-cause mortality rates to calculate the adjusted hazard ratios (HRs) and their corresponding 95% confidence intervals (95%CIs), considering potential confounding variables. Finally, a joint association between grip strength, obesity, and all-cause mortality was assessed.
RESULTS
During a median follow-up of 9.09±3.73 years, 135 adults with disabilities died. After adjusting all possible confounding variables, the HR of the group with the highest grip strength was significantly lower (HR: .36; 95% CI: .20-.65) than that of the group with the lowest grip strength. In the joint analysis, compared to the “weak and non-obese” group, the HRs (95% CIs) of all-cause mortality were .32 (.17-.62) and .27 (.10-.71) in the “strong and non-obese” and “strong and obese” groups, respectively.
CONCLUSION
High grip strength in Korean adults with disabilities aged ≥45 years was significantly associated with a lower all-cause mortality risk, independent of obesity. Hence, grip strength may be a simple indicator of mortality risk; however, additional research using large-scale survey data is required.
INTRODUCTION
People with disabilities generally have less access to medical services owing to physical or economic burdens and engage in fewer health behaviors than people without disabilities [1,2]. Hence, they have a higher risk of chronic disease morbidity and complications as well as higher mortality rates due to premature dementia and aging [3-6].
In Korea, the average life expectancy of people with disabilities is approximately 18 years shorter than that of people without disabilities. Furthermore, the difference is even greater for people with severe disabilities [7]. Therefore, various efforts are required to reduce the high mortality rate among people with disabilities compared with those without disabilities.
Grip strength, an indicator of total body muscle strength, is a clinically effective measurement tool as it is noninvasive and simple to measure [8]. According to recent epidemiological studies, low grip strength was associated with a high risk of developing chronic diseases, such as cardiovascular disease and metabolic syndrome. Furthermore, several studies also reported a significant association with a high risk of mortality [9-13].
However, most studies examine the relationship between grip strength and mortality risk among people without disabilities. Hence, these results may not be generalizable to people with disabilities. Compared to people without disabilities, people with disabilities often exhibit multiple disabilities or chronic conditions from an early age [9] and lower average grip strength across all age groups [10,11]. Therefore, the relationship between grip strength and mortality risk in people with disabilities may differ from that in people without disabilities. Although some studies reported a significant relationship between higher grip strength and lower mortality risk among people with disabilities [12,13], relevant research is lacking.
Obesity is a major risk factor of all-cause mortality. People who were obese had significantly higher mortality compared to non-obese people [14]. Furthermore, sarcopenic obesity, defined as low muscle strength or low muscle mass was significantly associated with a high all-cause mortality and had more strongly associated with a high all-cause mortality risk than obesity or low muscle strength alone [15,16]. Therefore, obesity may reinforce the association between lower grip strength and higher mortality in people with disabilities. However, physical fitness may be more important than obesity to survival of people with disability [17]. Therefore, it is necessary to investigate how obesity affects the association between grip strength and mortality in people with disability.
Therefore, this study aimed to examine the independent and joint association between grip strength and all-cause mortality with obesity in Korean adults with disability.
METHODS
1. Study population
This study used data from the Korean Longitudinal Study of Aging (KLoSA) conducted by the Korea Employment Information Service on middle-aged and older people. KLoSA employed a panel survey ap-proach to investigate their social, economic, psychological, demographic, and health status. The study aimed to derive valuable insights to shape socioeconomic policies. The KLoSA comprised a random sample of 10,254 adults aged 45 years or older, residing in Korea, except for Jeju Is-land. The same participants were followed up on every two years since the first survey (2006). Data for this study were extracted from the first to the seventh survey conducted in 2018 as part of the KLoSA. All surveys employed a computerized face-to-face interview method and included questionnaires on economic activity status, demographic information, disability information, vocational skills, and daily life-related items. The participants or their proxy responded to these questionnaires.
This study focused on 669 people with disabilities, who answered “ yes” to the question, “ Have you ever been diagnosed with a disability by a doctor?” out of 10,254 middle-aged and older people who participated in the first survey in 2006. Those who reported a history of cancer, cerebrovascular disease, and/or heart disease in the first survey (n=174), or whose death status was missing (n=65) were excluded. Finally, 430 participants were included.
2. Mortality ascertainment
Follow-up surveys from the second (2008) to the seventh survey (2018) were used to determine whether a participant had died and, if so, the date of death. If a participant died, the death status and date of death were investigated through proxy interviews. The date of death was obtained through a specific question: “ When was the date of death?”. Death status and date of death at follow-up were determined based on death certifi-cates and medical examiners’ reports.
3. Grip strength
Grip strength was measured using a dynamometer (NO6103; Tanita, Tokyo, Japan) with the elbows attached to the trunk and flexed at 90°. Final grip strength value was calculated as the overall average of two measurements of grip strength in the right and left hands. It was categorized into sex-specific tertiles (lowest, middle, and highest) based on the difference in grip strength between men and women [18-20].
4. Covariates
Age, sex, body mass index (BMI), smoking status, alcohol drinking status, educational level, household income, type of disability, regular exercise habits, history of hypertension and diabetes, and depression were used as covariates. All covariates were from the baseline survey. BMI was calculated from the weight and height of the participants. Smoking and alcohol drinking status were categorized according to their current smoking and alcohol drinking status, respectively. Education was categorized into four levels: elementary school or lower, middle school, high school, or college or higher. Household income was categorized as fol-lows: gross household income of <10 million won per year, <30 million won per year, or >30 million won per year. Marital status was categorized into unmarried, divorced/widowed/seperated, or married. Type of disability was categorized based on a doctor's diagnosis and included physical disability, brain lesion, visual impairment, hearing impairment, dysphagia, cardiac disorder, intellectual disability, developmental disability, or other disabilities. Regular exercise was defined as participation in exercise at least once per week. High blood pressure and diabetes were categorized based on diagnosis by a doctor. Depression was categorized based on questionnaire whether the participants had experienced depression consistently for two or more weeks in the past year.
5. Statistical analysis
Participants’ demographic characteristics were categorized according to sex-specific tertiles of grip strength. All continuous variables were presented as means and standard deviations, and categorical variables were presented as numbers and ratios. Differences between groups were ana-lyzed using analysis of variance and chi-squared tests. Survival time was calculated from the day of participation in the first survey to the day of death or the censor point.
The survival function based on the tertiles of grip strength was ana-lyzed using the Kaplan-Meier survival curve and log-rank test. The proportional hazards assumption was satisfied. To analyze the relationship between grip strength and all-cause mortality, HRs and 95% CIs were calculated using the Cox proportional-hazard model based on the low grip strength group.
Three models were used for analysis. Model 1 was not adjusted, and in Model 2, sex and age were adjusted. In Model 3, Model 2 was additionally adjusted for BMI, current smoking and alcohol status, education, household income, type of disability, regular exercise participation status, history of high blood pressure and diabetes, and depression. For sensitivity analyses, participants who died within one year of the first survey were excluded, and the results were compared.
To analyze the joint association of grip strength and obesity with all-cause mortality, we dichotomized grip strength to “ weak” (the lowest two-thirds) or “ strong” (the highest one-thirds), BMI to “ non-obese” (BMI <25 kg/m2) or “ obese” (BMI ≥25 kg/m2) [21]. And we categorized participants into “ weak and non-obese”, “ weak and obese”, “ strong and non-obese”, or “ strong and obese”. HRs and 95% CIs were calculated using the Cox proportional-hazard model based on the weak and non-obese group.
Missing grip strength data and covariates were imputed using the R package (“ mice”), and five replacement datasets were used. All statistical analyses were performed using R version 4.0.5. Statistical significance was set at p <.05.
RESULTS
Of the 430 participants, 135 died, and the mean follow-up period was 9.09 (±3.73) years. Participants’ demographic characteristics and categories according to the tertiles of grip strength are presented in Table 1. Their mean age was 63.2 years, and 57.7% were male. More than half of the participants had an educational background of elementary school or lower and an annual income of less than 10 million won. Most were physically disabled (64.2%), followed by those with visual (12.1%) and hearing impairments (8.8%).

Participants’ baseline characteristics by sex-specific grip strength tertiles
Categorization according to tertiles of grip strength revealed significant differences between the groups regarding age, BMI, smoking status, alcohol drinking status, education, house income prevalence of hypertension. However, no significant difference was found in sex, marital status, type of disability, participation in regular exercise, prevalence of diabetes and depression.
Table 2 presents the relationship between grip strength and the risk of mortality. In Model 1, confounding variables were not adjusted and the group with the highest grip strength showed statistically lower risk of mortality compared to the group with the lowest grip strength (HR, 0.22; 95% CI, 0.13-0.37). After adjusting for sex and age in Model 2, the HRs were increased slightly. However, the risk of mortality remained lower in the high grip strength group (HR, 0.38; 95% CI, 0.22-0.66). In Model 3, the results remained consistent after adjusting for all potential confounders (HR, 0.36; 95% CI, 0.20-0.65). Furthermore, even after all the confounding variables were adjusted, the risk of mortality decreased by approximately 5% for every 1-kg increase in grip strength (HR, 0.96; 95% CI, 0.94-0.99).
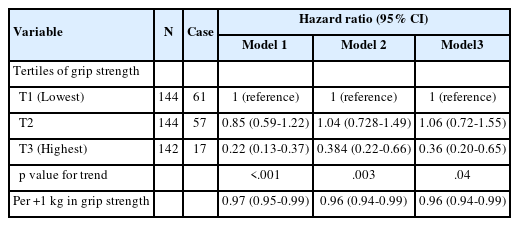
Hazard ratios and 95% confidence intervals of all-cause mortality by tertiles of grip strength
For sensitivity analysis, three participants who died within one year after the first survey were excluded. The relevance was slightly lower; however, the risk ratio of the high grip strength group remained lower than that of the low grip strength group (HR, 0.53; 95% CI, 0.29-0.96).
A joint association of grip strength and obesity with all-cause mortality was shown in Fig. 1. Compared to weak and non-obese group, the weak and obese group, the strong and non-obese group, and strong and obese group had lower HR of all-cause mortality with HRs (95% CIs) of all-cause mortality were 0.32 (0.17-0.62) and 0.27 (0.10-0.71).

A joint association of grip strength and obesity of all-cause mortality.
DISCUSSION
To the best of our knowledge, this is the first study to investigate the relationship between grip strength and mortality risk in Koreans with disabilities. We investigated the relationship between grip strength and all-cause mortality in Korean adults aged 45 years or older with disabilities via data from the KLoSA. A total of 430 people with disabilities were followed up for an average of 9.05 years, and 135 people died during the survey period.
Analysis of the all-cause mortality risk according to sex-specific grip strength tertiles, revealed that high grip strength was significantly associated with a low risk of mortality. In addition, a strong association existed, even after the confounding variables such as sex, age, type of disability, income level, and chronic disease were excluded. Hence, these results indicated that high grip strength was associated with a lower risk of mortality in people with disabilities.
Our findings were in line with a meta-analysis conducted on people without disabilities, where grip strength consistently emerged as a strong predictor of mortality [22,23]. In addition, two previous studies that investigated the relationship between grip strength and mortality risk in people with disabilities reported a significant relationship [12,13]. These results support our finding on a significant association between grip strength and mortality risk in people with disabilities.
Low muscle strength was associated with decreased performance in activities of daily living, which could explain the association between grip strength and mortality. People with low muscle strength had difficulty performing activities of daily living, which limited additional activities [24]. Lack of physical activity is a major risk factor of injuries and diseases, and mortality [25], additional decline in muscle strength, and sarcopenia [26]. In a study on older women with disabilities, those with low muscle strength were more inactive, whereas active older women with disabilities had relatively higher muscle strength [27]. Thus, low muscle strength in people with disabilities indicated a poor ability to perform activities of daily living, which could be related to high mortality from physical inac-tivity.
Additionally, we investigated to examine how the association between grip strength and all-cause mortality is modified by obesity, a strong risk factor of mortality. As a result, grip strength was strongly associated with all-cause mortality regardless of obesity. Our findings were consistent with previous studies with people without disability [28,29]. Regardless of obesity status, high grip strength was significantly associated with low mortality risk.
Interestingly, the obese and strong group had a lower risk of mortality than non-obese and strong group. BMI is strongly correlated with skeletal muscle mass and is also related to nutritional status [30,31]. Therefore, BMI of ≥25 kg/m2 may reflect higher muscle mass and better nutritional status in people with disabilities than lower BMI. In fact, it was found that the mortality risk of elderly with disability with a BMI of ≥25 kg/m2 was significantly lower than those of normal weight [32], and these results were also found in studies on people without disability [14]. However, the BMI used to classify obesity status in this study does not accu-rately reflect the percentage of body fat, abdominal visceral fat, and lean mass, which are related to actual chronic diseases. To confirm the clear effect of obesity on the relationship between grip strength and mortality, follow-up studies considering body fat percentage, abdominal visceral fat, and lean body mass should be conducted in the future.
Sarcopenia, a syndrome characterized by an overall loss of muscle and skeletal muscle mass is a leading cause of muscle loss during aging. In people with disabilities, sarcopenia was more prevalent and occurred from a younger age. Hence, they were more easily exposed to low muscle strength than people without disabilities, and were at a higher risk [33,34]. The prevalence of sarcopenia in Korean adults with cerebral palsy was approximately 48%, more than four times higher than that in adults without disabilities [34]. Therefore, people with disabilities had lower muscle strength on average across all age groups [10,11].
Our participants showed significantly low grip strength. Their average grip strength was 29.0 kg for men and 17.8 kg for women, which was less than 5% of the grip strength of Korean adults aged 40 years and older [35]. Moreover, considering that the grip strength criterion for diagnosing sarcopenia was less than 26 kg for men and 18 kg for women, most people with disabilities fell under the range for sarcopenia. Therefore, continued efforts are required to prevent, maintain, and increase muscle strength in people with disabilities.
Our study's strength was that it was the first to longitudinally investigate the association between grip strength and mortality through a long-term follow-up. However, this study has several limitations. First, the study only included Koreans with disabilities who participated in the KLoSA; therefore, the results is not generalizable to the global population. Second, most of the data, apart from grip strength measurement values, were col-lected through subjective questionnaires, leading to possible bias due to non-response.
High grip strength was associated with lower mortality in Korean adults with disabilities. These findings underscore the importance of maintaining an optimal muscle strength for the health and survival of people with disabilities. Future studies should use large-scale survey data to identify the key variables that affect this association.
CONCLUSIONS
In this pioneering study, we investigated the relationship between grip strength and mortality risk among Korean adults with disabilities aged 45 years and older. Our finding demonstrated a compelling association, indicating that higher grip strength was linked to a significantly reduced all-cause mortality risk in this population.
Notes
All parts of the research were performed by the contributing author.
AUTHOR CONTRIBUTIONS
Conceptualization: SH Yim; Data curation: SH Yim; Formal analysis: SH Yim; Funding acquisition: SH Yim; Methodology: SH Yim; Project administration: SH Yim; Visualization: SH Yim; Writing - original draft: SH Yim; Writing - review & editing: SH Yim.