운동선수의 비타민D에 대한 최신지견
Recent Advance on Vitamin D in Athletes
Article information

Abstract
PURPOSE
Vitamin D plays important roles in calcium homeostasis and bone metabolism. Since vitamin D receptors (VDRs) are located in a variety of organs, including skeletal muscle, vitamin D has potentially widespread effects. The purpose of this review was to summarize the current understanding of the effects of vitamin D on muscle function and exercise performance in athletes.
METHODS
In this narrative review, we summarized previous studies by searching the literature in the PubMed, Google Scholar, and Science Direct databases.
RESULTS
Vitamin D has been shown to regulate multiple actions in skeletal muscle tissue, such as myocyte proliferation and growth via genomic and non-genomic molecular pathways. Higher levels of vitamin D are associated with improved skeletal muscle function and exercise performance. Moreover, in some studies, vitamin D supplementation has beneficial effects on muscle strength in athletes, especially those who are vitamin D-deficient.
CONCLUSIONS
Vitamin D appears to have beneficial effects on muscle and exercise performance in athletes. However, more studies are needed to clarify the action and dosage of vitamin D in athletes.
서 론
최근 전 세계적으로 혈중 비타민 D 부족 유병률이 높은 것으로 보고되고 이와 더불어 비타민 D 부족과 다양한 질병이 연관되어 있는 것으로 보고되고 있다[1,2]. 비타민 D는 칼슘 대사에 영향을 미쳐 골 건강과 밀접한 관련이 있는 것으로 주로 연구되어 왔으나 최근에는 근 기능(muscle function), 심혈관 기능(cardiovascular function), 염증 반응(immune function) 및 골격근 조절(musculoskeletal function)에도 역할을 하는 것으로 보고한다[3–5].
비타민 D는 단백질 합성(protein synthesis)과 속근 섬유 증가와도 관련성이 있어 근력(muscle strength)과 운동수행능력(performance)에 영향을 미친다는 연구 결과가 보고되고 있다. 또한 비타민 D 결핍은 운동선수들의 부상률 증가와도 관련성이 있다고 보고하여 운동선수에게 비타민 D 수준은 고려되어야 할 의학적 지표인 것으로 사료되지만 이와 관련하여 명확히 규명되어 있지 않다. 한편, 일반인뿐만 아니라 운동선수들에게도 비타민 D 결핍이 흔한 것으로 보고되는데 최근 우리나라 선수들을 대상으로 한 연구에 의하면 실내 종목, 여자 선수, 나이가 많은 선수, 체질량지수가 높은 선수 등에서 비타민 D 수치가 낮은 것으로 보고했다[6]. 따라서 운동 선수들은 적절한 혈중 비타민 D 수준을 유지하고 비타민 D 보충제 섭취하는 것에 대한 보다 세심한 정보가 필요할 것으로 사료된다.
이에 본 종설에서는 운동선수에서 비타민 D 수준과 근력 및 경기수행능력과 연관성 및 비타민 D 보조제 효과에 대해 최근 연구 동향들을 정리해 보았다.
연구 방법
1. 자료수집
본 종설의 작성을 위해 ‘PubMed’, ‘Google Scholar’, ‘Science Direct da-tabases’와 같은 학술 검색 시스템을 활용하여 연구 논문을 자료로 수집하였다. 검색 키워드는 ‘vitamin D’, ‘vitamin D and muscle strength’, ‘vitamin D and athletic performance’, ‘vitamin D and athletes’ 등으로 문헌을 검색하였다.
결 과
1. 비타민D 합성과 대사
비타민 D는 체내에서 합성되어 혈액을 통해 순환하며 목표 조직으로 전달되어 다양한 기능을 조절하기 때문에 호르몬으로 인식되기도 한다. 사람에게는 동물에서 합성되는 비타민 D3 (cholecalciferol)와 식물에서 합성되는 비타민 D2 (ergocalciferol) 두 가지 형태의 비타민 D가 주로 존재한다[7]. 비타민 D는 음식 혹은 보조식품을 통해서도 합성이 되지만 대부분은 햇빛을 통해 7-디하이드로콜레스테롤(7-dehydro-choleterol)이 피부에서 비타민 D3로 전환되어 합성된다. 음식 섭취를 통해 혹은 피부에서 합성된 비타민 D3은 간에서 효소 CYP2R1에 의해 비활성 전구체인 25-hydroxyvitamin D3 (calcidiol)로 전환되고, 이는 신장에서 효소 CYP27B1에 의해 활성 호르몬인 비타민 D (1,25-dihy-droxyvitamin D, 1,25 (OH) D)로 전환되어 작용한다[8,9].
비타민 D는 25 (OH) D와 1,25 (OH) D의 형태로 혈액을 순환한다. 우리가 보통 측정하는 혈중 비타민 D 농도는 비활성 호르몬인 25 (OH) D 분자의 농도를 나타내는데, 25 (OH) D 분자의 경우 반감기가 15일인 반면 활성 호르몬인 1,25 (OH) D의 경우 반감기가 4시간으로 짧기 때문에 활성형 비타민 D의 전구체인 25 (OH) D 농도로 측정한다[10]. 내분비 학회 지침에 따르면(Endocrine Society's clinical guideline) 25 (OH) D 농도가 20 ng/mL 이하인 경우 결핍, 21-29 ng/mL의 경우 부족/불충분, 30 ng/mL 이상을 적정수준으로 정의한다(Table 1) [11].

대부분의 영양소는 적절한 음식 섭취로 체내에 필요한 양을 공급받을 수 있지만 비타민 D의 경우는 음식 섭취로 인해 우리 몸에 필요한 최소량(10%)만 공급되고 대부분은 햇빛(90%)을 통해 공급받는다. 비타민 D를 함유하고 있는 음식으로 지방질이 풍부한 생선, 우유, 버섯 등이 있지만 우리 몸에 필요한 만큼의 충분한 양을 함유하고 있지 않다[8]. 따라서 운동선수들의 경우 특히 햇빛에 많이 노출되지 않는 실내 종목 선수들의 경우 비타민 D 하루 권장량을 충족하기 위해서 비타민 D가 함유된 보조제를 섭취하는 것이 적정수준의 비타민 D 농도를 유지할 수 있는 방법으로 판단된다. 그러나 비타민 D의 과량 섭취는 체내 비타민 D의 지나친 증가를 초래하여 고칼슘뇨증과 혈액의 칼슘 농도를 높여 다양한 조직에 칼슘 침착을 일으킬 수 있기 때문에 비타민 D 보조제 섭취 양에 대해 주의를 기울여야한다[12].
2. 골격근에서 비타민D의 역할
비타민 D는 부갑상샘 호르몬(parathyroid hormone, PTH)과 함께 칼슘(Ca2+)과 인(P)의 항상성 조절을 통해 뼈의 발달과 성장 및 뼈와 관련된 질병에 관여한다[13]. 혈중 칼슘 농도가 감소하게 되면 부갑상샘 호르몬이 자극되고 이는 비타민 D를 활성형 비타민 D로 전환시켜 장과 신장에서 칼슘 흡수를 증가시키고 뼈 흡수(bone resorption) 등의 작용을 자극하는 것이 가장 일반적인 역할로 알려진다. 최근 비타민 D는 단백질 합성(protein synthesis)에도 관여하는 것으로 보고된다[14,15]. 비타민 D는 비타민 D 수용체(vitamin D receptor, VDR)을 활성화하면서 기능을 하는데 비타민 D 수용체는 뼈, 신장, 장관점막, 지방조직, 폐, 췌장뿐만 아니라 근육세포에서도 존재하여 비타민 D가 부족할 경우 골격근 발달도 영향을 주는 것으로 보고되고 있다[16]. 선행 연구에 의하면 사람의 근육세포에서 비타민 D 수용체가 존재하고 근육 세포에 활성형 비타민 D가 흡수되는데 비타민 D 수용체가 중요한 역할을 하는 것을 확인하였다[17].
비타민 D와 비타민 D 수용체는 유전자적 효과(genomic effect)와 비유전자적 효과(non-genomic effect)를 통해 근육세포에 작용한다[18] (Fig. 1). 활성형 비타민 D는 핵과 세포막에 존재하는 수용체를 통해 직접적 혹은 간접적인 방법으로 흡수되어 그 기능한다. 활성형 비타민 D 는 비타민D 수용체와 결합한 후 retinoid receptor (RXR)와 결합하여 1,25 (OH) D/VDR/RXR 복합체를 형성한 뒤 핵 내로 들어가(translo-cated) 비타민 D 반응영역(vitamin D response elements, VDRE)과 결합한 뒤 유전자의 전사(transcription) 활성화에 영향을 주며 유전자적 효과를 내는 것으로 보고된다[18]. 예를 들어, 1,25 (OH) D/VDR/RXR 복합체는 인슐린유사성장인자-1 (insulin-like growth factors-1, IGF-1)를 자극하여 근육세포의 분화와 속근 섬유(type 2 muscle fiber)의 증식을 촉진시키고, 또한 칼모듈린(calmodulin)을 자극하여 근 수축을 향상시킨다고 보고한다[14]. 또한 활성형 비타민 D는 세포막에 있는 비타민 D 수용체와 결합하여 비유전자적 효과를 통해 세포 내에 다양한 역할을 한다. 세포막에 비타민 D 수용체와 결합한 활성형 비타민 D는 Src활성화를 통해 MAPK (mitogen-activated protein kinase)를 자극하여 근육세포의 증식과 성장을 자극한다[19]. 또한 활성형 비타민 D의 비유전자적 경로는 칼슘 이온의 세포 내로 유입, 칼슘 이온의 세포내 외 수준의 조절, 인(phosphorus)이 함유된 화합물의 항상성 조절 및 부갑상샘 호르몬 분비 자극 등에 영향을 주는 것으로 보고된다[14]. 즉, 활성형 비타민 D는 비타민 D 수용체와 결합을 통해 직간접적으로 골격근의 부피 증가, 근력 증가 및 근육 수축력 증가에 영향을 미칠 수 있는 것으로 판단된다.

The actions of vitamin D with genomic and non-genomic effects. VDR, vitamin D receptor; VDRE, Vitamin D response elements; RXR, reti-noid-X receptor.
비타민 D가 골격근에 미치는 영향에 대한 조절 기전은 동물 연구와 임상연구를 통해 제안되고 있다. Braga et al. [20]의 연구에 의하면 마우스 근육에서 분리한 골격근 위성세포에 활성형 비타민 D를 처치했을 때 MYOD1 (myogenic differentiation 1), MYOG (myogenin) 등의 발현이 증가하는 것으로 나타났고 이는 근관 세포의 형성과 마이오스타틴(myostatin)의 발현이 감소되는 것으로 나타났다. 이와 유사하게 VDR이 전신에서 제거된 마우스 모델(whole-body VDR knockout mice model)에서 근섬유의 크기와 근력이 감소되는 것을 확인하였고[21,22], 근육에서만 VDR이 제거(muscle-specific VDR knockdow model)되었을 때에도 근육세포의 성장 및 분화가 둔화되는 것을 확인하였다[23]. 임상연구에서는 근 손상 후 VDR 발현이 증가되어 근 재생(regeneration)과 연관성이 있는 것으로 보고하였으며[24] 단기 저항성 운동 후 VDR 단백질 수준이 1-3시간 이내에 증가하는 것으로 확인되었다[25]. 이는 AKT/mTOR 신호전달의 증가는 인슐린/류신(insulin/leucine)의 동화작용(anabolic stimulation) 강화 및 인슐린 수용체 발현(insulin receptor)을 증가시켜 단백질 합성을 증가시키는 것으로 보고했다[26].
한편, 비타민 D 부족은 근육조직의 구조적 병리학적 문제를 일으킬 수 있는 것으로 보고한다. 비타민 D가 부족한 경우 근육조직에 섬유사이 공간(interfibrillar space)이 확장되어 있었고 지방 침윤 및 섬유화가 관찰되는 것으로 보고했다[27]. 또한 속근 섬유의 경우 비타민 D 수준과 직접적인 상관관계가 있는 것으로 보고한다. 그 예로 Oh et al. [28]등의 연구에 의하면 366명의 어깨 질환이 있는 사람을 대상으로 혈중 비타민 D 수준과 연관성을 분석해 보았을 때 낮은 수준의 비타민 D는 어깨 근육의 지방변성증가와 관련성이 있는 것으로 나타났고, 등속성 근력(isokinetic muscle torque) 감소와 상관관계가 있는 것으로 나타났다. 즉, 비타민 D는 근육세포에서 단백질 합성 등에 영향을 미치고 이는 근육조직의 크기, 수축력 및 근력 등과 상관관계가 있는 것으로 보고되기 때문에 운동선수들의 경기력에도 영향을 미칠 것으로 사료된다. 특히, 비타민 D 수용체는 앞서도 언급했듯이 다양한 조직에서 발현하고 있는데 골격근뿐만 아니라 심장 근육(cardiac muscle)과 혈관 조직(vascular tissue)에도 발현하기 때문에 비타민 D는 심혈관계 시스템에 산소를 포함한 혈액 공급에 영향을 줄 것으로 판단된다[29]. 따라서 혈중 비타민 D 부족을 정상 수준으로 치료하는 것은 심근의 기능 향상과 골격근의 산화 능력 향상에 관련성이 있을 것으로 판단되고[30,31]이는 선수들의 운동 능력에 중요하게 작용될 것으로 판단된다.
3. 혈중 비타민D 수준과 근력 및 운동수행능력과의 관계
전 세계적으로 혈중 비타민 D 결핍 혹은 부족을 겪고 있는 사람이 10억명 정도 되는 것으로 보고되며[1] 우리나라의 경우 국민건강영양조사자료에 따르면 비타민 D 수준이 30 ng/mL 이하인 성인 남성은 약 86.8%, 여성은 약 93.3%가 비타민 D 결핍 혹은 부족 현상을 겪는 것으로 보고된다[32]. 국내 운동선수의 경우 비타민 D 평균 수치가 비운동선수에 비해 높게 나타났지만, 비타민 D 농도가 32 ng/mL 이하로 결핍 혹은 부족 상태인 선수가 약 80%로 나타났고 실내 종목, 여자 선수, 나이가 많은 선수, 체질량지수가 높은 선수일수록 비타민 D 수치가 낮게 나타나고 있어 비타민 D 부족현상은 운동 선수들에게도 예외가 아니다[33].
최근 선행연구에서 혈중 비타민 D수준과 운동선수의 근력과 관련성에 대해 횡단적 연구를 통해 분석하여 보고하였다(Table 2). Hildebrand 등은 대학 운동선수들을 대상으로 비타민 D와 근력과의 상관관계에 대해서 분석한 결과 혈중 비타민 D가 28 ng/mL 이하인 경우 수직 점프 (vertical jump), 스쿼트 점프(squat jump) 감소와 유의한 연관성이 있는 것으로 나타났다[34]. 이와 유사하게 축구 선수들과 대학생 선수들 대상으로 비타민 D 수치와 근력의 상관관계를 분석한 결과 스쿼트 점프, 반동 점프(countermovement jump), 스프린트(sprint)와 같은 근력과 유의한 양의 상관관계가 있는 것으로 나타났다[35–39]. 위의 결과들을 종합해보면 비타민 D 수치가 충분할 경우 근력과 양의 상관관계가 있는 것으로 나타났고 그 중에서도 점프 능력과 상관관계가 높은 것으로 보고했다. 이와 관련된 메커니즘은 비타민 D농도가 높을수록 비타민 D 수용체를 활성화를 증가시켜 근육량 증가[40], 신경근 협응 능력 증대[41] 및 속근 섬유의 단면적을 넓혔을 것으로 예상된다. 특히, 속근 섬유[42] 및 신경근 협응 능력 증대[43]는 점프 및 스프린트 능력과 연관성이 있다고 보고된다. 따라서 적정수준의 비타민 D는 근력과 긍정적인 상관관계에 영향을 미쳤을 것으로 사료된다.
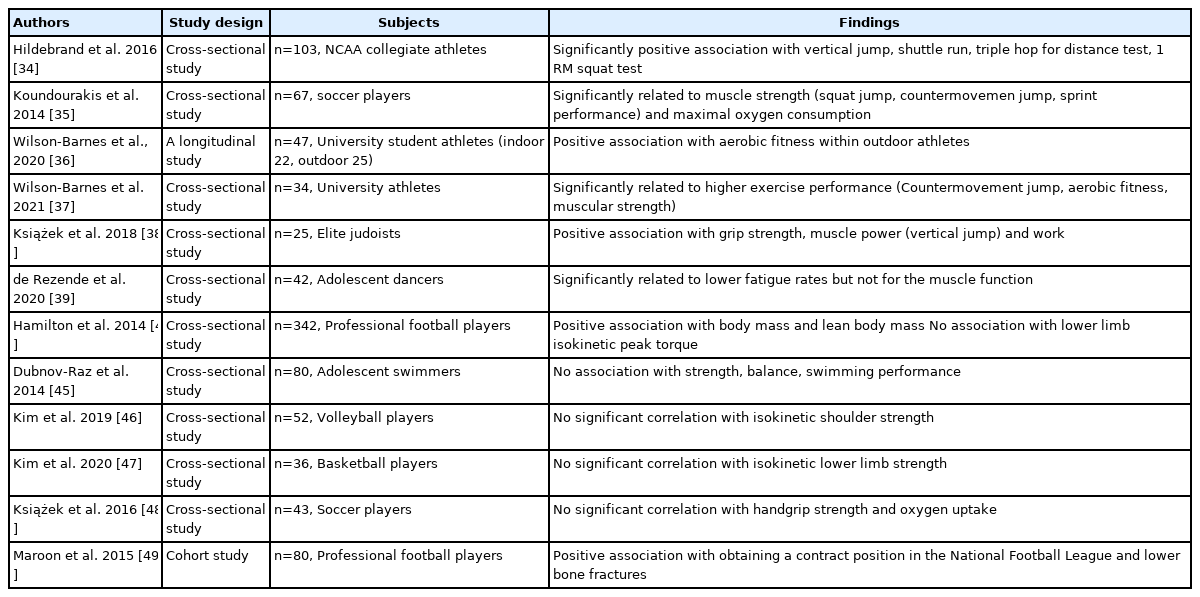
Association between vitamin D level and muscle strength and physical performance
한편, 비타민 D수치가 근력과 무관하다는 연구보고도 되고 있다. Hamilton et al. [44]은 미식축구 선수들의 비타민 D 수치와 제지방양과 양의 상관관계가 있는 것을 확인하였지만 하지 근력과 상관관계는 없는 것으로 보고하였고, 이와 유사하게 Dubnov-Raz et al. [45]의 연구에서도 청소년 수영선수들의 비타민 D 수준은 악력과 관련성이 없는 것으로 보고하였다. Kim et al. [46,47]은 배구와 농구 남자 선수들을 대상으로 비타민 D가 결핍과 상지 및 하지의 근력과의 연관성을 분석하였다. 그 결과 배구와 농구 선수들에서 비타민 D 결핍이 흔하게 나타났지만 비타민 D 결핍이 상하지 근력 모두에서 유의한 상관관계는 관찰되지 않는 것으로 보고했다[46,47]. 또한 Książ ek et al. [38]은 유도 선수들을 대상으로 비타민 D와 근력, 수직 점프 및 일 양(work)이 유의한 양의 상관관계를 갖는다고 보고하였지만, 축구선수들을 대상으로 한 연구에서는 악력과 유산소성 능력에 비타민 D수준이 연관성이 없는 것으로 보고하였다[48]. 이러한 결과는 상대적으로 적은 피험자 숫자로 인해 유의한 상관관계를 밝히지 못한 것으로 사료되며, 종목과 근력 측정 부위에 따라서 결과가 상이 했을 것으로 판단된다. 또한 비타민 D 수치가 제지방양과 유의한 상관관계가 있다는 점은 선수들의 근골격계 건강에 비타민 D가 중요한 역할을 한다는 점을 시사한다.
혈중 비타민 D 수치는 운동수행능력과도 연관성이 있는 것으로 보고하였다. Maroon et al. [49]은 미국 프로 축구선수들을 대상으로 비타민 D 수치와 프로 계약을 맺을 수 있는 능력과 상관관계를 조사하였다. 그 결과 비타민 D 수준이 높은 선수들이 비타민 D 수준이 낮은 선수들에 비해 최소 1회 이상 골절율(bone fracture)이 낮고 프로 계약을 맺을 확률이 높은 것으로 나타났다[49]. 이는 적정수준의 비타민 D로 인해 부상에 대한 위험이 감소하고 이는 운동수행능력에 긍정적으로 영향을 준 것으로 저자는 제언하였다.
인간의 비타민 D 수용체는 염색체 12q13에 위치하고 있고, TaqI, BsmI, ApaI, FokI 등의 다형성(polymorphism)이 존재하는 것으로 알려진다. 선행연구에서 비타민 D 수용체 유전자 다형과 근력과의 연관성에 대해 분석하였고, BsmI, ApaI 유전자 형은 근력과 유의한 상관관계가 있는 것으로 나타났다[50,51].
위의 결과들을 종합하여 보면 운동선수의 비타민 D 수준과 근력 및 운동수행능력에 대해 상반된 연구 결과들로 인해 현재까지 명확한 결론을 내릴 수 없다. 이는 비타민 D 부족 정의, 비타민 D 부족 지속 정도, 측정 계절, 비타민 D 수용체 다형성 등 다양한 요소들이 연구 결과에 영향을 미쳤을 것으로 사료된다. 따라서 추후 위의 요소들을 고려한 중재 연구를 통해 명확한 결과를 도출해야 할 것으로 판단된다.
4. 비타민D 보조제 섭취와 운동수행능력
비타민 D 보조제는 근육의 비타민 D 수용체 발현을 증가시켜 근육의 기능을 향상시키고 뼈 골절율을 감소시킨다는 보고는 주로 노인들을 대상으로 이루어져왔다[52,53]. 최근 비타민 D 수준의 중요성이 운동 선수들에게도 강조되면서 비타민 D 보조제가 운동선수의 근력과 운동수행능력에 미치는 영향에 대한 연구가 보고되고 있다(Table 3). Wyon et al. [54]은 발레 선수들을 대상으로 비타민 D 수치가 상대적으로 감소되는 겨울시즌에 16주간 매일 2,000 IU 비타민 D 보조제를 섭취하도록 하는 전향적 관찰 연구를 실시하였다. 그 결과 비타민 D 보조제 섭취는 비타민 D 보조제를 섭취하지 않은 그룹에 비해 등속성 근력이 약 18.7%, 수직 점프가 약 7.1% 유의하게 향상시키는 것으로 나타났다. 또한 실험 기간 동안 비타민 D 보조제를 섭취한 그룹은 그렇지 않은 그룹에 비해 부상 횟수도 유의하게 감소된 것으로 나타났다[54]. Wyon et al. [55]의 또 다른 연구에서는 유도 선수들을 대상으로 겨울철 1회성 급성 비타민 D 보충제 섭취가 근력에 미치는 효과에 대해 분석한 결과 150,000 IU 비타민 D 보조제를 하루에 섭취 후 근력이 약 11% 증가된 것을 확인하였다. Jung et al. [56]은 태권도 선수들을 대상으로 겨울철 하루 5,000 IU씩 4주간 비타민 D를 섭취하게 한 결과 무릎의 근력이 유의하게 증가된 것을 확인하였다. Close et al. [57]은 영국 운동선수들을 대상으로 겨울 시즌에 8주간 비타민 D 보조제를 하루 5,000 IU씩 섭취하도록 중재하였다. 8주간 중재 후 혈중 비타민 D 수치를 측정한 결과, 위약 그룹(placebo)은 혈중 vitamin D 수준이 변함없었던 반면, 중재 그룹은 혈중 비타민 D 수준이 사전 11.6±10.0 ng/mL에서 41.3±10.0 ng/mL로 유의하게 증가된 것을 확인하였다. 혈중 비타민 D 수준의 증가와 함께 10 m 스프린트 시간과 수직 점프 기록이 유의하게 향상되어 비타민 D 보조제는 선수들의 운동수행능력에 긍정적인 영향을 주는 것으로 보고했다. 위의 선행연구들을 종합해보면, 겨울철 충분한 햇빛을 공급받지 못할 경우 선수들의 비타민 D 부족 현상은 더욱 심화될 것으로 예상된다. 이때 보조제 섭취를 통해 적정수준의 비타민 D 수치 유지는 근력 및 운동수행능력의 감소를 억제하고 이와 더불어 선수들의 부상을 예방할 수 있을 것으로 사료된다.
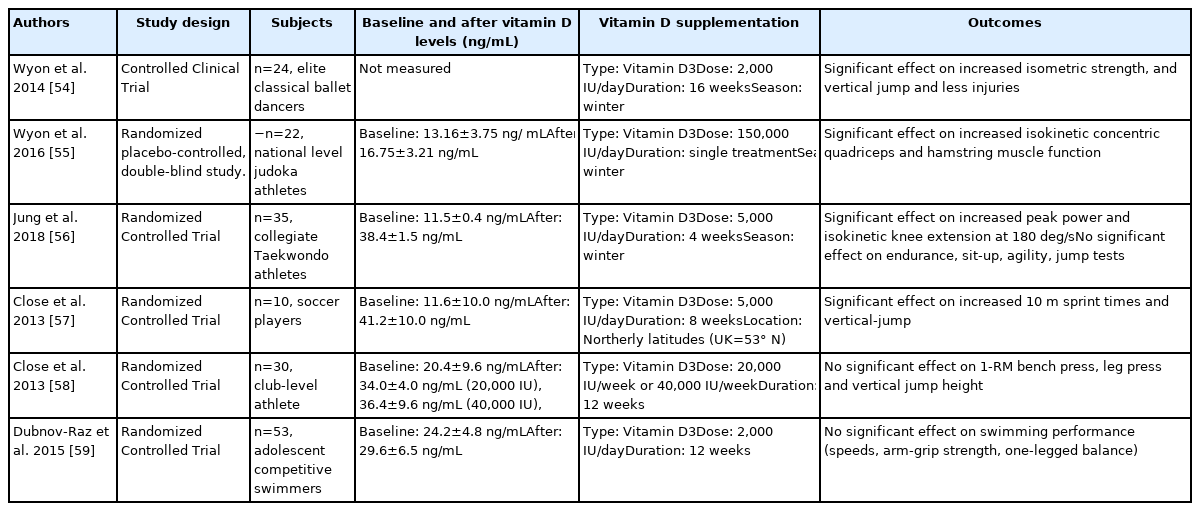
Vitamin D supplementation on muscular function and physical performance in athletes
한편 Close et al. [58]은 또 다른 연구에서 클럽선수들을 대상으로 주당 20,000 IU 혹은 40,000 IU 농도의 비타민 D 보조제를 12주간 섭취하도록 하였다. 혈중 비타민 D 농도는 주당 20,000 IU 혹은 40,000 IU를 섭취한 그룹 모두에서 혈중 비타민 D 농도가 30 ng/mL 이상으로 증가하여 비타민 D 보조제 섭취 양에 상관없이 사전에 비해 사후에 유의하게 증가하는 것으로 나타났다. 그러나 운동수행능력의 경우 보조제 섭취로 혈중 비타민 D 농도가 증가했음에도 불구하고 유의한 변화가 없는 것으로 나타났다. 이는 그룹 당 10명의 선수들을 대상으로 실험하여 표본 크기(sample size)가 적었던 점, 클럽선수들을 대상으로 한 점이 전문 선수들을 대상으로 한 이전 연구와 다른 결과를 도출하게 된 연구의 제한점으로 사료된다[57,59]. 따라서 비타민 D 수치가 부족 혹은 결핍인 운동 선수들의 경우 하루 최소 2,000 IU 이상 비타민 D 보조제를 6주 이상 섭취하게 되면 혈중 비타민 D 수준이 최소 30 ng/mL 이상 도달 할 것으로 예상된다. 그러나 비타민D 보조제 과다 복용은 체내 칼슘 농도를 증가시켜 다양한 조직에 칼슘 침작을 일으킬 수 있기에 섭취 용량에 주의하고 주기적인 체크가 필요하다.
또한 다양한 연구에서 비타민 D 보조제 섭취와 근력 및 운동수행능력 향상과의 관련성에 대해 보고하였지만 연구 대상자의 성별, 실험 전 기준선의 비타민 D 농도, 섭취한 비타민 D의 복용 용량, 복용 계절 및 기간에 따라 연구결과가 상의한 것으로 판단된다. 추후에는 많은 피험자와 무작위 배정 임상시험(randomized controlled trial, RCT) 디자인을 통해 보다 명확한 연구결과를 도출해야 할 것으로 사료된다.
5. 비타민D2와 비타민D3 보조제
우리가 섭취하는 비타민 D 보조제는 비타민 D2(식물성)와 비타민 D3(동물성)의 형태가 있다. 비타민 D2와 비타민 D3은 유사한 하이드록실화(hydroxylation)를 거쳐 활성화 비타민 D 형태로 전환되지만 혈중 비타민 25 (OH) D 수준에 영향을 미치는 정도는 다른 것으로 보고된다[60,61]. Nieman et al. [60]의 연구에서는 전문 운동선수들을 대상으로 비타민 D2 보조제를 하루 3,800 IU를 섭취하게 하여 총 6주간 중재한 후 근력 및 근육의 피로도 정도를 측정하였다. 그 결과 6주간 중재는 혈중 25 (OH) D2의 수준을 통계학적으로 유의하게 증가시켰으며 25 (OH) D3은 유의하게 감소시켰다. 또한 근육 기능과 관련된 운동수행능력은 유의한 변화가 없는 것으로 나타났다. 과거에는 비타민 D2와 비타민 D3의 효과에 대한 구분이 없는 것으로 간주되었으나 최근 연구에 의하면 비타민 D2는 비타민 D3에 비해 혈중에서 농도 유지에 효율성이 떨어져 비타민 D2 기능에 영향을 미치는 것으로 나타났다[62]. 즉, 비타민 D3이 비타민 D2에 비해 혈중 비타민 D 농도 유지에 더 유리하기에 선수들의 운동수행능력 향상에 더 효과적일 것으로 판단된다.
결 론
비타민 D는 스테로이드 호르몬의 일종으로 칼슘의 항상성 조절과 골 대사를 포함하여 다양한 기능을 한다. 비타민 D 수용체는 다양한 세포에서 발현되고 있고 특히 근육세포에서 유전자적 혹은 비 유전자적 신호전달을 통해 근육세포의 증식과 성장을 촉진하는 것으로 보고한다. 이러한 세포 신호 전달은 적정 수준의 비타민 D 수치일 때 근골격계 건강뿐만 아니라 근력 및 운동수행능력 향상에 긍정적인 영향을 미칠 것으로 판단된다. 그러나 비타민 D 보충제와 운동선수의 근육 기능에 대한 상이한 연구 결과도 보고되고 있어 비타민 D 보충제 권고에 대해 여전히 불확실한 면이 존재하기에 추후 보충제 섭취 정도, 비타민 D의 형태, 비타민 D 부족에 대한 정확한 정의 등이 필요할 것으로 판단된다.
Notes
이 논문 작성에 있어서 어떠한 조직으로부터 재정을 포함한 일체의 지원을 받지 않았으며, 논문에 영향을 미칠 수 있는 어떠한 관계도 없음을 밝힌다.
AUTHOR CONTRIBUTION
Conceptualization: J Cho, H Song; Data curation: J Cho, S Park; Project administration; J Cho; Visualization; J Cho; Writing-original draft: J Cho, S Park; Writing-review & editing: J Cho, S Park, H Song.