Grip Strength Measurement in the Right Hand Better Predicts Mortality Regardless of Dominant Hand
Article information

Trans Abstract
Purpose
Muscle strength is often higher when measured on the dominant hand than on the non-dominant hand, and there are reports of differences in the mortality rates between left-handed and right-handed people in the Korean population. Therefore, it is necessary to longitudinally investigate the effect of grip strength of the dominant hand on mortality rates.
Methods
Data from the Korean Longitudinal Study of Aging (KLoSA) from 2006 to 2016 were assessed and 9,196 research subjects were included. The effect of grip strength on mortality rates were analyzed by measuring 1) the right hand, 2) the left hand, and 3) the dominant hand for right-handed and left-handed people. In addition, the association between grip strength and mental health disorders were analyzed and a generalized estimating equation (GEE) model was used.
Results
The association between grip strength and all-cause mortality was statistically significant in both hands. When the grip strength was measured with the right and left hands, the log likelihood ratio test for the Akaike information criterion (AIC) of both hands for mortality was significant (p=.018). When the grip strength for the left-handed people was measured with the right and left hands, the log likelihood ratio test for the AIC of both hands for mortality was significant (p=.009). Taken together, there was no difference in mortality between right-handed and ambidextrous individuals according to the measurement of right-handed and left-handed grip, but left-handed individuals had a higher mortality according to the measurement of right-handed grip than that of the left hand, which is the dominant side.
Conclusions
Therefore, there was no difference in mortality rates according to the dominant hand, and the measurement of grip strength in the right hand was a better predictor of mortality than the use of maximum or average value after measuring grip strength in both hands.
INTRODUCTION
Muscle function is important for maintaining optimal health and physical performance throughout life [1,2]. Previous studies have reported that muscle function affects diabetes [3], plasma lipids [4], sudden cardiac death risk [2], and all-cause mortality [3].
However, muscle function declines with age due to changes in body composition over time, such as a decrease in lean body mass and an increase in fat mass [4]. Skeletal muscle, a major component of lean body mass, plays a role in regulating body function and power generation. However, the decrease in lean body mass due to aging, along with loss of skeletal muscle mass and strength, leads to a decrease in daily life physical activities in elderly individuals and causes disability, frailty, and falls. This loss of muscle mass is related to structural and functional changes. Additionally, decreased muscle strength in the elderly increases the risk of cardiovascular disease and mortality and all-cause mortality [5].
Hand grip strength is correlated with the whole body's muscle strength and has been suggested as an indicator for muscular function in the elderly's upper extremity and frailty [6]. Grip strength, a surrogate indicator of muscle strength, is simple, inexpensive, and easily used[13,14]. Growing evidence suggests that changes in the skeletal muscle measured using grip strength represent changes in biological vitality and body function with aging [7]. Low grip strength is thought to be associated with disability, morbidity, and mortality [8]. Contrastingly, previous studies have reported that increased grip strength leads to lowered cardiovascular disease, mortality, and frailty risks [5].
Although many studies have suggested that grip strength is an index of predicting disease prevalence and mortality, inconsistencies have been reported in the relevance of mortality prediction and the method of grip strength measurement. Reportedly, grip strength level is a better predictor for mortality than the rate of grip strength change [9]. Accelerated loss of grip strength was found to be a better predictor for mortality than the level of grip strength [10].
Additionally, previous studies report a relationship between grip strength and disease prevalence and mortality; however, there are few studies conducted with Korean individuals. Kim et al. [11] showed that low grip strength is an independent indicator of mortality in the elderly, and Park et al. [12] reported that depression and low grip strength increase mortality in the elderly. Additionally, Bae et al. [13] also reported that the mortality rate among individuals over the age of 65, with rapidly decreasing grip strength over time, is higher than that of the elderly whose grip strength declines slowly. However, a survey of adults over 45 years of age and the elderly showed a weak association between low grip strength and mortality, indicating that the association between grip strength and mortality in Koreans is still unclear.
The grip strength test entails squeezing a dynamometer as strongly as possible with one hand to measure the isometric muscle strength [14]. Most studies measured grip strength using the maximum or average value after using both hands for the measurement [10]. Generally, muscle strength is often higher when measured in the dominant hand [15]. Ap-proximately 5.7% of Koreans are reportedly left-handed, and there are reports of differences in the mortality rate between left-handed [16], and right-handed people [17]. In general, the reported difference in muscle strength between the dominant and non-dominant hand among right-handed people is approximately 10% [18], and that among left-handed individuals is small [19]. Additionally, the suggested cutoff value of weak hand grip strength in Koreans is 16.8 kg for women and 28.9 kg for men [20]. For every 5 kg decrease from the initial measured value, all-cause mortality reportedly increased by 16% [21]. Therefore, it is necessary to investigate the effect of the dominant hand's grip strength on mortality rates because changes in the grip strength of the dominant hand can in-fluence mortality.
Therefore, we conducted this study to determine the measurement and use of grip strength to increase the validity and reliability of predicting mortality. We analyzed the effect of grip strength on mortality rates by measuring the strengths of the 1) right hand, 2) left hand, and 3) dominant hand for right-handed and left-handed people.
METHODS
1. Data source
The data used for the following analyses were derived from the Korean Longitudinal Study of Aging (KLoSA) performed by the Korea Labor Institute. KLoSA is composed of 7 categories such as population, family, health, employment, income, wealth, subjective expectation and life expectation as biennial survey from 2006 to 2016. As a type of study that possesses both the strengths of cross-sectional data and time series data, the KLoSA was constructed by repeatedly surveying the identical con-tent for the same respondents. Thus, all variables included in the KLoSA were repeatedly measured from the 1st wave to the 6th wave to capture longitudinal trends of the observed variables. Participants were selected randomly using a multistage, stratified probability sampling design to create a nationally representative sample of community-dwelling Korean adults aged 45 years and older. In case of refusal to participate, another subject was selected from an additional, similar sample from the same district. In this study, 9,196 participants were included in the analysis at baseline, excluding those with missing values for the variables of interest.
2. Dependent variable
All-cause mortality during the time interval from year 2006 to the end of follow-up was the main outcome of the study. Death over a maximum follow-up period of 10 years was determined by death certificates.
3. Independent variable
Handgrip strength was measured using a dynamometer (Hand Grip Meter 6103, Tanita, Tokyo, Japan) to the nearest 0.1 kg. Participants stand with lower their arms to the side and their feet at shoulder width apart. Participants were required to grip the bar with their second finger and hold the dynamometer with each hand as hard as they could. The both hand sides were examined twice and used the average values.
4. Control variable
In terms of factors that affect all-cause mortality in middle-aged and aged participants, age, gender, education level, residential region, income, smoking status, alcohol consumption, marital status, social engagement, number of chronic diseases, and body mass index (BMI) were considered. Specifically, in terms of chronic diseases, Hypertension, diabetes, cancer, chronic obstructive pulmonary disease, liver disease, cardiovascular disease, cerebrovascular disease and arthritis were included.
5. Statistical analysis
In this study, using 2006 as the baseline year and considering the fol-low-up period until 2016, the chi-squared test, Kaplan-Meier survival analysis and Cox proportional-hazards models were used to analyze the association between grip strength and all-cause mortality. The Cox pro-portional-hazard model was used to calculate the adjusted hazard ratio (aHR) and 95% confidence intervals (CI), to assess the effects of grip strength on mortality. Survival time was the outcome variable, which was measured as the time-interval between the date of enrollment and date death or censoring (up to 10 years). Kaplan-Meier survival analysis and the log-rank test were used to evaluate the cumulative incidence of all-cause mortality, with respect to grip strength. All statistical tests were two-tailed, with the null hypothesis of no difference being rejected if p <.05. Statistical analysis was performed using SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA).
RESULTS
1. Sample characteristics
Baseline general characteristics of participants are shown in Table 1. Out of the 9,196 participants gathered at baseline, 3,117 (33.9%) participants were reported as Low group and among them, 702 (22.5%) were reported as death. In terms of grip strength of right and left hand in Low group, 685 (23.4%) participants and 718 (21.6%) were reported as death. In terms of frequently used hands, 1,249 (16.7%) participants in grip strength measured on right-handed were reported as death and 44 (16.1%) participants in grip strength measured on left handed were reported as death. General characteristics of socioeconomic status and health status and risk behavior variables are also listed in Table 1.

General characteristics of participants at baseline
2. Relationship between grip strength and all-cause mortality
In the fully adjusted model (Table 2), the association between grip strength and all-cause mortality was statistically significant in both hands, with the following Hazard ratio (HR) predicting increased mortality rate: OR=1.919 (p <.0001, AIC [Akaike information criterion: 26,205]) for Low group in grip strength measured on right hand, OR= 1.916 (p <.0001, AIC: 26,210]) for Low group in grip strength measured on left hand vs. high grip strength. When the grip strength was measured with the right and left hands, respectively, the log likelihood ratio test for the AIC of both hands for mortality was significant (p−value: .018).
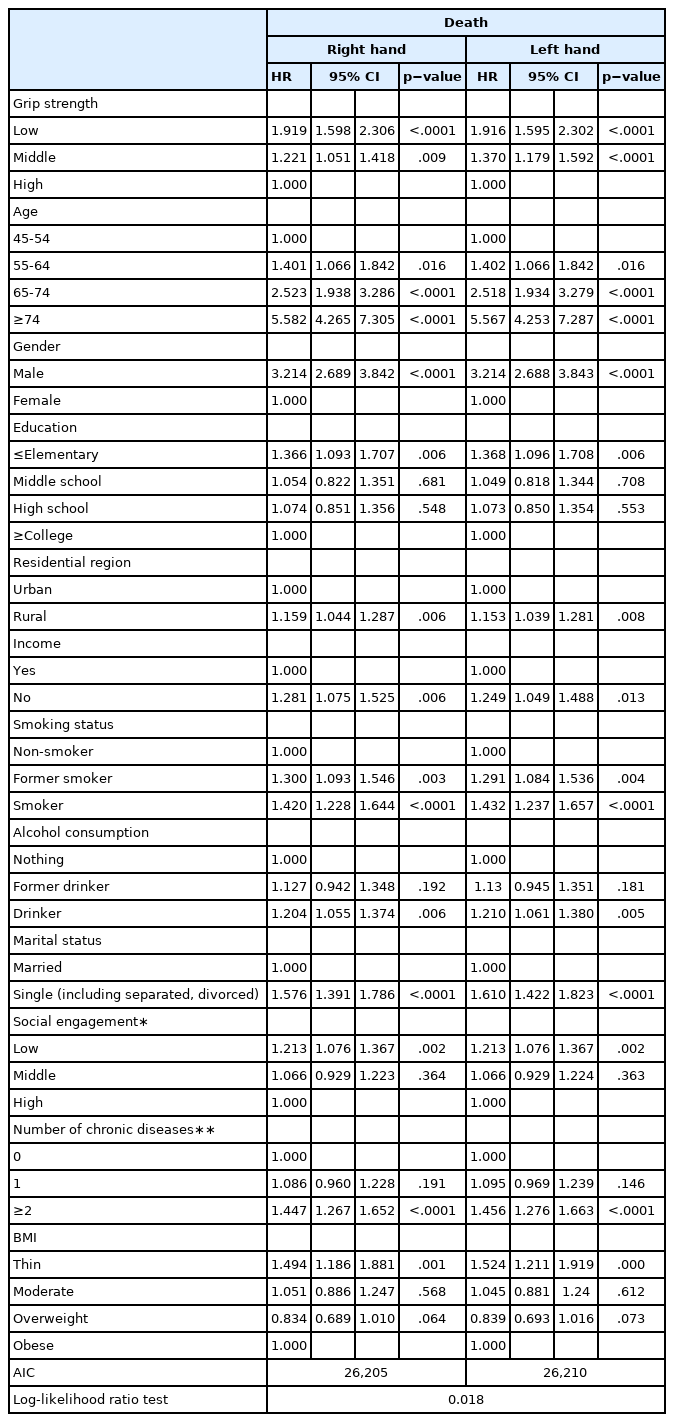
Adjusted effect of grip strength on death
3. Relationship between grip strength and all-cause mortality by frequently used hands
Table 3 shows the association grip strength and all-cause mortality by frequently used hands and log-likelihood ratio test was performed to verify the difference in model fit between both hands. When the grip strength for right-handed people was measured with the right and left hands, the log likelihood ratio test for the AIC of both hands for mortality was not significant (p−value: .148) and there was no difference in the results for the ambidextrous (p−value: .400). However, when the grip strength for left-handed people was measured with the right and left hands, the log likelihood ratio test for the AIC of both hands for mortality was significant (p−value: .0009).
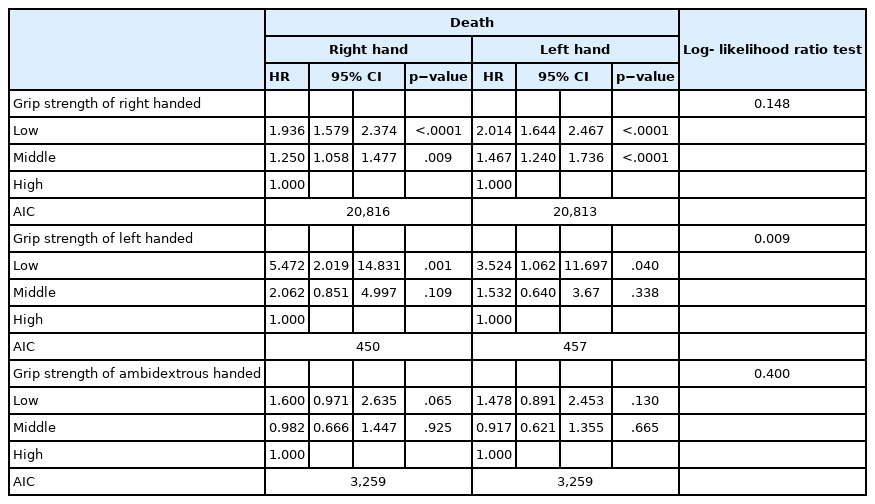
Adjusted effect of grip strength of frequently used hands on death
DISCUSSION
Low grip strength in middle and older ages is reportedly associated with future disability [22], cardiovascular disease [5], and increased risk of complications [23]. Additionally, for every 5 kg decrease in grip strength compared to the initial measured value, the all-cause mortality increases by 16%, and the risk of cause-specific mortality between the ages of 35 and 70 increases by 7-17% [21].
In a study of Korean subjects, Kim et al. [24] demonstrated that low grip strength in postmenopausal women is associated with low bone density and increased risk of future fragility fractures. Shim & Yoo [25] reported that for each 1 kg increase in grip strength, the 10-year cardiovascular disease risk decreases. However, Lee et al. [26] pointed out that grip strength increase is associated with a decreased cardiovascular disease risk in young and middle-aged individuals, but not in the elderly; therefore, it is necessary to look at the health implications over a long period of time, preferably throughout life. In this study, we found that low grip strength influenced mortality rate (p <.001), with a higher mortality rate among right-handed and left-handed individuals with middle and low grip strength compared to individuals with high grip strength (p <.001). Alternatively, there was no significant difference in the mortality rate according to the grip strength of the dominant hand.
Mortality is affected by demographic factors (e.g., age and gender), socioeconomic variables (e.g., income, education, employment, and marital status), lifestyle and health behaviors (e.g., smoking and alcohol consumption), and health statuses (e.g., chronic disease and BMI) [9]. In this study, mortality rate increased with age, men, the lower the level of education, rural residents, current and previous smokers, former drinker, one existing disease, and lower or higher BIM index. After adjusting all variables that affect the relationship between grip strength and mortality, the risk of mortality in right-handed people with low and medium grip strength increased. For left-handed people, the risk of mortality increased by quartiles compared to those of people with middle and high grip strength. In the case of ambidextrous persons, the risk of mortality some increased, but the relevance was weaker. Kim et al. [11]. reported a similar result that individuals with low grip strength increased the cause-specific mortality in men, but women. Taken together, the association between the right hand's grip strength and the mortality rate was high, regardless of the dominant hand.
In general, grip strength is measured using the dominant hand, and the maximum value is used as the index. This is because, reportedly, the dominant hand has approximately 10% higher grip strength than the non-dominant hand [27]. However, Petersen et al. [19] reported that about 20% (61 per 310 persons) of cases showed no difference between the grip strength of the non-dominant and dominant hand. When com-paring grip strength between the two hands, the difference was 12.72% in the case of the right-handed people, but 0.08% in the case of left-handed people, indicating that the 10% difference rule in grip strength between the dominant and non-dominant hands does not apply. Reportedly, the number of left-handed individuals decreases with age; as per previous studies, left-handed individuals were required to adjust while living in a right-handed world or had a shorter lifespan [28].
The reasons for the shorter lifespan of left-handed individuals have been suggested by several studies. In addition to the problems of right-handed tools used by left-handed people, most of the workflow and ar-rangement of workspaces are implicitly designed for right-handed indi-viduals. Left-handed workers who are not adapted to this are more likely to suffer from injury and experience a decrease in work efficiency [29]. Although there are differences among studies, the probability of getting injured in car accidents has been reported to be as high as 55%, while using tools has been reported to be as high as 54%, and while doing house-work has been reported to be as high as 49% [30]. These results may explain why left-handed individuals have a higher mortality rate than right-handed individuals; however, these results cannot explain the findings of our study wherein grip strength of the right hand in left-handed individuals did not correlate with mortality.
A recent study demonstrated that the grip strength of the dominant hand has a strong relationship with muscle size in the forearm and that the increase in muscle size of the dominant hand may result from muscle contraction during asymmetric hand motions, such as carrying a weight with one hand, throwing a ball, or grasping a racket during sports [15]. The 1-cm difference between the forearm-ulna and the fore-arm-radius muscle thickness corresponds to a 14.9 kg and 17.1 kg difference in grip strength, respectively [15]. The criterion for distinguishing between left-handed and right-handed Koreans is to throw a ball or use a knife or scissors. Therefore, it is likely that a left-handed person per-forms more asymmetric hand movements with the left hand. However, the muscle thickness of the forearm was not measured in this study, and hence, there is a limitation of not knowing whether left-handed individ-uals have thicker right forearms.
Finally, a high correlation between right-handed grip strength and mortality in left-handed individuals may be deduced by the fact that the proportion of left-handed individuals is 79% in those under 30 years of age; however, this proportion is lower in those over 30. Additionally, 44.1% of individuals feel uncomfortable in their daily lives, and as age increases, the proportion of those feeling less or no discomfort increases compared to younger individuals [16]. Therefore, since this study was conducted on a sample of individuals aged over 45 years, it is possible that as they age, they will be more likely to use the right hand as they are adapted to using right-handed instruments or tools. For this reason, it can be assumed that left-handed individuals showed a higher mortality rate according to the measurement of right-handed grip strength than the left-handed grip, which is the dominant side.
Several limitations must be considered when interpreting our findings. First, the methods used to characterize HGS vary considerably with regards to the choice of dynamometer or the measurement protocol. Second, control variable in this study, can be inaccurate and the potential for biased can be reported since it is surveyed using self-reported questionnaire. Fourth, this study was conducted on the Korean population, and there are limitations in generalizing the results to other races. Nevertheless, to our knowledge, this is the first longitudinal design study to evaluate the association between grip strength and mortality in Korean middle aged population.
CONCLUSION
Mortality is affected by vary factors, such as age, gender, socioeconomic variables, smoking and alcohol consumption habitues, and health statuses. There was no difference in mortality corresponding to the use of the dominant hand in right-handed and ambidextrous individuals. However, left-handed individuals showed a higher mortality according to the measurement of right-hand grip strength than that of the left hand, which is the dominant side. Therefore, there was no difference in mortality according to the dominant hand, and as a result, the level of grip strength in the right hand was found to be the most appropriate index for mortality prediction, regardless of the dominant hand.
Notes
No author has any other conflict of interest to declare.
AUTHOR CONTRIBUTION
Conceptualization: JH Kim; Data curation: JH Kim; Formal analysis: JH Kim; Funding acquisition: JH Kim; Methodology: JH Kim; Project administration: JH Kim, YA shin; Visualization: YA Shin, WH Choi; Writing-original draft: YA Shin; Writing-review&editing: JH Kim, WH Choi.