성공적인 노화를 위한 혈류제한 운동
Abstract
PURPOSE
Generally, an increase in life expectancy is accompanied by various geriatric diseases. However, there is a possibility that geriatric diseases can be prevented and improved through exercise. Exercise is recommended for older adults, but high-intensity exercise (HIE) increases the risk of potential injury. Therefore, blood flow restriction exercise (BFRE) is attracting attention as an alternative for older people who cannot perform HIE. However, mechanisms underlying the physiological effects and benefits of BFRE in older adults have not yet been fully elucidated. This study aimed to summarize the effects of BFRE on aging-related physiological changes and examine its applicability as an effective intervention for successful aging.
METHODS
A literature search of electronic databases, including PubMed, Web of Science, and Google Scholar, was conducted for literature published between January 1, 2000, and December 31, 2022.
RESULTS
BFRE can effectively increase muscle mass and strength in older adults. Chronic BFRE improved blood pressure, vascular function, and arterial compliance. Although BFRE did not induce changes in bone mineral density (BMD) and cognitive function, positive effects were shown by increasing bone formation markers and neurotrophic factors expression. Relatively, the risk of side effects of BFRE was very low, and even older patients with cardiovascular diseases appeared to have no risk.
CONCLUSIONS
This review confirms that BFRE can be an effective and safe intervention to increase muscle mass and strength and improve cardiovascular function. Moreover, BFRE can potentially improve BMD and cognitive function in older adults. In conclusion, BFRE can be an effective intervention for successful aging; additional follow-up studies are needed.
Keywords: Successful aging, Older adults, Blood flow restriction, Exercise
색인어: 성공적인 노화, 노인, 혈류제한, 운동
서 론
최근 의료기술의 발달, 위생수준의 향상, 건강관리에 대한 관심 확대 등으로 인해 인간의 기대수명(life expectancy)이 과거에 비해 증가하고 있다[ 1]. 하지만 단순한 기대수명의 증가는 노화로 인한 심혈관계 질환(cardiovascular disease) 및 신경퇴행성 질환(neurodegenerative disease) 등 다양한 질병을 동반하며, 이는 개인 및 사회의 경제적, 심리적 부담을 증가시킨다[ 1- 3]. 최근에는 기대수명의 증가 뿐만 아니라 질환이나 장애 없이 양호한 건강 상태로 살아가는 기간을 의미하는 건강수명(healthy life year)의 중요성도 높아지고 있다[ 4]. 하지만 세계보건기구(World Health Organization, WHO) 보고에 따르면 건강수명의 증가는 기대수명의 증가를 따라가지 못하고 있으며[ 5], 이러한 격차를 해소하기 위해 성공적인 노화(successful aging)가 중요하다. 성공적인 노화란 노화에 따른 부정적인 신체적 변화를 완화시키거나 지연시키는 것으로, 질병에 대한 위험을 줄이며, 독립적인 생활이 가능한 신체능력과 인지능력을 유지하는 것을 의미한다[ 6, 7]. 성공적인 노화를 위한 비약물적 전략(non-drug strategy) 중 하나인 운동은 노화에 따른 심혈관계 및 신경퇴행성 질환 등 다양한 질환의 발병 위험을 감소시킬 뿐만 아니라 신체기능의 유지 및 발달에 효과적인 방법이다[ 8- 11]. 미국스포츠의학회(American College of Sports Medicine, ACSM)의 권고 사항에 따르면 건강 유지를 위해 주당 150분 이상의 중강도 유산소 운동 혹은 주당 60분 이상의 고강도 유산소 운동과 함께 근육 강화를 위한 주 2회 이상의 저항성 운동을 권장하고 있다[ 12]. 하지만 노인들에게 높은 강도의 운동은 관절통(joint pain)이나 근육좌상(muscle strain)과 같은 부작용을 유발할 수 있으며, 심혈관계에도 부담을 줄 수 있으므로 노년층에게는 새로운 운동 전략의 적용이 필요하다[ 13- 16]. 고강도의 운동을 하기 어려운 경우 혈류제한(blood flow restriction, BFR) 운동이 새로운 대안이 될 수 있다. 혈류제한 운동은 사지 근위부(proximal of the limbs)에 압력 커프(cuff)를 착용하여 혈류를 제한시킨 후 운동을 하는 방법으로 저강도 저항성 운동으로도 고강도 저항성 운동과 유사한 근육 비대 효과를 얻을 수 있다고 알려져 있다[ 17, 18]. 혈류를 제한하는 경우 혈류제한 부위에 국소적인 저산소(hypoxia), 허혈(ischemia) 상태가 유발되며[ 19, 20], 근육 단백질 합성을 자극할 수 있는 대사 스트레스(metabolic stress)가 증가한다[ 21- 23]. 혈류제한 운동은 고강도의 운동을 할 수 없는 개인에게 적용 가능한 운동방법으로 주목받고 있으며, 근골격계 질환자 및 재활환자 등 특수한 집단에게 주로 적용되고 있다[ 24- 26]. 혈류제한에 관한 연구는 주로 저항성 운동과 결합되어 골격근 및 근력 증가에 초점이 맞춰져 왔다[ 19]. 하지만 노인들의 근골격계, 심혈관계 및 신경퇴행성 질환과 같은 노화와 관련된 질환들을 예방 및 개선하기 위한 혈류제한 운동의 생리적 효과와 이점에 대한 기전은 아직 명확하게 밝혀지지 않은 실정이다. 또한 혈류제한 운동은 혈관을 압박하여 심혈관계의 부담을 증가시킬 수 있기 때문에[ 27], 젊은 성인에 비해 상대적으로 높은 혈압을 가지고 있는 노인에게 잠재적인 위험성이 존재할 수 있다[ 28]. 따라서 본 종설(review)에서는 노화와 관련된 생리적 변화와 이에 대한 혈류제한 운동의 효과와 안전성을 검토하고 성공적인 노화를 위한 효과적인 운동 중재 방법으로 혈류제한 운동 프로그램의 적용 가능성을 고찰하고자 한다.
연구 방법
1. 자료 검색 및 수집
2000년 1월부터 2022년 12월까지 출판된 문헌들을 학술 검색 시스템인 “ Web of Science, “ PubMed”, “ Google Scholar”를 이용하여 본 종설을 위한 자료수집을 실시하였다. 자료 조사는 ‘ blood flow restriction or Kaatsu or vascular occlusion’, ‘ elder or older or aging or ageing’, ‘ muscle strength or muscle mass’, ‘ bone mineral density or bone mineral content’, ‘ cardiovascular or cardiac or vascular’, ‘ cognitive’ or executive or brain’ 등의 키워드를 조합하여 실시하였다. 또한 본 종설에서는 성공적인 노화를 위한 혈류제한 운동의 효과를 알아보기 위하여 포함 및 제외 기준을 다음과 같이 정하였다.
1) 포함기준(Inclusion Criteria)
노화로 인한 생리적 변화는 50세 이후로 급격하게 진행된다는 선행 연구를 참고하여 50세 이상의 피험자를 대상으로 한 연구를 포함하였으며[ 29, 30], 무작위 교차 시험(randomized crossover) 및 무작위 대조 시험(randomized controlled trial)으로 진행된 연구를 포함하였다. 또한 비교군에도 운동 중재를 실시한 문헌을 분석에 포함하였다.
2) 제외기준(Exclusion Criteria)
연구 대상자의 연령이 50세 미만이거나, 무작위 교차 연구 및 무작위 대조 연구를 제외한 단일군 연구, 동물 연구, 종설 연구, 메타분석 연구는 본 연구의 범위를 벗어나므로 제외하였다. 또한 운동 중재 방법이 명확하지 않은 연구, 운동 중재가 포함되지 않은 단순 혈류제한 연구, 한국어와 영어 이외의 언어로 작성된 문헌은 제외하였다.
연구 결과
1. 혈류제한 운동의 효과
1) 혈류제한 운동의 골격근 및 근력에 대한 효과
골격근은 20-30세에 최고점(maximum)에 도달한 뒤, 10년에 약 3-8% 정도 감소하기 시작하며, 50-60세 이후로는 10년에 약 5-10%로 감소 폭이 커지게 된다[ 31, 32]. 이는 노화에 따른 신체활동의 감소와 함께 근성장에 영향을 미치는 인슐린(insulin), 테스토스테론(testoster-one), 성장호르몬(growth hormone, GH), 인슐린유사성장인자(insulin-like growth factor-1, IGF-1)와 같은 호르몬 수준의 감소 및 인슐린 저항성 증가, Interleukin-1β, TNF-α, Interleukin-6 등과 같은 전염증성 사이토카인(pro-inflammatory cytokine)의 증가를 포함하는 내분비 기능의 변화로 설명될 수 있다[ 33]. 또한 노화에 따라 근육성장과 관련된 Pro-tein kinase B (Akt)/mammalian target of rapamycin (mTOR) 관련 신호 전달체계가 약화되어 골격근의 감소는 더욱 심화된다[ 34]. 근력 또한 나이가 증가함에 따라 점진적으로 감소하며, 근력의 감소는 골격근의 감소보다 2-5배 정도 더 큰 감소폭을 나타낸다[ 35]. 노화와 관련된 근육의 양적 및 질적 변화는 근감소증(sarcopenia)으로 이어지게 된다[ 36]. 근감소증은 낙상 및 신체기능 장애, 삶의 질 저하와 관련이 있으며[ 37], 신경퇴행성 질환, 심혈관계 및 호흡기 질환 등 다양한 질환의 발병률과 사망률 증가와도 관련이 있다[ 38- 41]. 따라서 노년기에 적절한 골격근과 근력을 유지하거나 증가시키는 것은 건강한 삶을 영위하는데 매우 중요하다. 혈류제한 운동이 노인들의 골격근 및 근력에 미치는 효과에 관한 선행연구를 종합한 내용은 Table 1에 제시하였다. 자료분석에 포함된 연구 중 한 개의 연구를 제외하고[ 42], 최대근력(1 repetition maximum, 1RM)의 20-30%의 저강도 저항성 운동에 혈류제한을 적용하는 경우, 동일한 강도의 일반적인 저강도 저항성 운동보다 더 큰 골격근 증가가 나타났다[ 25, 43]. 또한 혈류제한 저강도 저항성 운동을 통한 골격근의 증가는 고강도 저항성 운동과 유사한 수준이었다[ 25, 44- 46]. 근력 또한 1RM의 20-30%의 저강도 저항성 운동에 혈류제한을 적용하는 경우 동일한 강도의 일반적인 저항성 운동보다 근력 증가에 효과적이었으며, 혈류제한 저강도 저항성 운동을 통한 근력 증가는 고강도 운동과 유사한 수준으로 관찰되었다[ 25, 43- 45, 47- 49]. 흥미로운 것은 혈류제한을 통해 저강도 유산소 운동으로도 골격근의 증가가 보고되었다는 점인데, Abe et al. [ 50]의 연구에 따르면 6주간의 혈류제한 저강도 유산소 운동을 통해 골격근의 증가가 보고되고 있으며, Kargaran et al. [ 51]과 Ozaki et al. [ 52, 53]의 연구에 따르면 8-10주간의 혈류제한 저강도 유산소 운동은 골격근 뿐만 아니라 근력 증가에도 효과적이었다. 이는 걷기 운동과 같은 저강도 유산소 운동도 혈류제한의 적용을 통해 노인들의 골격근과 근력의 증가를 유도할 수 있다는 것을 의미한다.
Table 1.
Effects of low intensity exercise with blood flow restriction on muscle mass and strength
|
Author |
Subjects |
Group |
Intervention |
Results |
|
Frequency |
Intensity |
Volume |
Type |
|
Abe et al., 2010 [50] |
Old adults (n=19, 60-78 yr) |
Walk
Walk+BFR |
6 wks, 5 times/wk |
67 m/min |
20 min |
Walk |
Girth↑
CSA↑
MM↑ |
|
Cook et al., 2017 [45] |
Old adults (n=36, 75.6 yr) |
CON
LIT+BFR
HIT |
12 wks, 2 times/wk |
1RM 30, 50%
1RM 70% |
3 sets, until failure |
Resistance exercise |
CSA↑
Strength↑ |
|
Ferraz et al., 2018 [25] |
Old women (n=48, 50-65 yr) |
LIT
LIT+BFR
HIT |
12 wks, 2 times/wk |
1RM 30%
1RM 80% |
4-5 sets, 15 reps
4-5 sets, 10 reps |
Resistance exercise |
CSA↑
Strength↑ |
|
Karabulut et al., 2009 [47] |
Old men (n=37, 50-64 yr) |
CON
LIT+BFR
HIT |
6 wks, 3 times/wk |
1RM 20%
1RM 80% |
3 sets (30/15/15 reps)
3 sets, 8 reps |
Resistance exercise |
Strength↑ |
|
Kargaran et al., 2021 [51] |
Old women (n=24, 62.9±3.1 yr) |
CON
DT
DT+BFR |
8 wks, 3 times/wk |
HRR 45% |
20 min |
Walk+CT |
Strength↑
MQ↑ |
|
Kim et al., 2017 [16] |
Old adults (n=23, 60-80 yr) |
LIT+BFR
HIT |
4 wks, 3 times/wk |
MVC 20%
MVC 75% |
3 sets, until fatigue |
Handgrip |
Girth↑
Grip strength↑ |
|
Letieri et al., 2018 [43] |
Old women (n=56,68.8±5.09 yr) |
CON
LIT
LIT+LBFR
LIT+HBFR HIT |
16 wks, 3 times/wk |
1RM 20-30%
1RM 70-80% |
3-4 sets, 15 reps
3-4 sets, 6-8 reps |
Resistance exercise |
Strength↑ |
|
Libardi et al., 2015 [44] |
Old adults (n=25, >60 yr) |
CON
HIT
LIT+BFR |
12 wks, 4 times/wk |
1RM 70-80%
1RM 20-30% |
4 sets, 10 reps
4 sets (30/15/15/15 reps) |
Combined training |
CSA↑
Strength↑ |
|
Linero et al., 2021 [48] |
Old women (n=26, 50-60 yr) |
CON
LIT
LIT+BFR
MHIT |
12 wks, 3 times/wk |
1RM 30%
1RM 60-80% |
3 sets, 20 reps
3 sets, 10 reps |
Resistance exercise |
Strength↑ |
|
Ozaki et al., 2011a [52] |
Old adults (n=23, 57-76 yr) |
Walk
Walk+BFR |
10 wks, 4 times/wk |
HRR 45% |
20 min |
Walk |
CSA↑
Strength↑ |
|
Ozaki et al., 2011b [53] |
Old adults (n=18, 57-73 yr) |
Walk
Walk+BFR |
10 wks, 4 times/wk |
HRR 45% |
20 min |
|
CSA↑
MM↑
Strength↑ |
|
Pereira Neto et al., 2018 [49] |
Old women (n=20, >50 yr) |
CON
AT+BFR
LIT+BFR
HIT |
12 wks, 2 times/wk |
HRmax 65%
1RM 30%
1RM 80% |
15 min
4 sets, until failure |
Walk Resistance exercise |
Strength↑ |
|
Silva et al., 2018 [42] |
Old women (n=18, 62.28±5.07 yr) |
LIT+BFR
HIT |
16 wks, 2 times/wk |
1RM 30%
1RM 70% |
4 sets, 15 reps
3 sets, 10 reps |
Resistance exercise |
MM ↔ |
|
Vechin et al., 2015 [46] |
Old adults (n=23, 59-71 yr) |
LIT+BFR
HIT |
12 wks, 2 times/wk |
1RM 20-30%
1RM 70-80% |
4 sets (30/15/15/15 reps)
4 sets, 10 reps |
Resistance exercise |
CSA↑
Strength ↔ |
저강도 혈류제한 운동으로 유발되는 파스포크레아틴(phosphocre-atine, PCr)의 고갈, 무기 인산염(inorganic phosphate, Pi)의 증가, 젖산(lactate)의 축적과 근육의 산도(pH) 저하는 대사스트레스를 증가시킨다[ 21, 54]. 이는 근성장과 관련된 테스토스테론이나 GH, IGF-1 등의 호르몬의 발현을 증가시키며[ 54- 56], 골격근 합성의 주요 조절 인자인 Akt/mTOR 신호전달체계를 활성화시킬 수 있다[ 57, 58]. 또한 혈류를 제한하는 경우 지근 섬유(type I muscle fiber)에 대한 산소 공급이 불충분해지기 때문에 낮은 강도에서도 속근 섬유(type II muscle fiber)의 활성화를 유도할 수 있다[ 59]. 노화에 따른 골격근의 감소는 주로 속근 섬유에서 이루어진다는 것을 고려했을 때[ 60, 61], 혈류제한 운동을 통해 속근 섬유의 활성화를 유도할 수 있다는 것은 혈류제한 운동이 노인들의 근감소증 예방 및 개선에 효과적인 운동 중재방법으로 제안될 수도 있음을 의미한다. 이외에도 혈류제한 운동은 상대적으로 낮은 운동강도로 진행되기 때문에 노인들의 관절이나 뼈에 가해지는 부담이 덜 하다는 장점 또한 가지고 있다[ 62].
2) 혈류제한 운동의 골밀도 및 골표지자(bone turnover marker)에 대한 효과
골밀도는 뼈 조직에 있는 무기질의 밀도(bone mineral density)로 평가되며, 뼈의 강도를 나타내는 지표다. 골밀도를 측정하는 방법으로는 이중에너지방사선흡수법(dual-energy X-ray absorptiometry, DEXA), 전산화단층촬영법(computed tomography, CT), 초음파(ultra sound), 자기공명영상(magnetic resonance imaging, MRI), 방사선 측량법(X-ray ra-diogrammetry) 등이 있다[ 63]. 하지만 골밀도의 변화는 오랜 기간에 걸쳐 이루어지기 때문에 골밀도의 변화를 예측할 수 있는 생화학적 마커인 골표지자를 소변이나 혈액에서 평가하기도 한다[ 64]. 골표지자는 골의 생성을 나타내는 골형성표지자(bone formation marker)와 골의 분해를 나타내는 골흡수표지자(bone resorption marker)로 나뉘게 되며, 골형성표지자의 경우 alkaline phosphatase (ALP), osteocalcin, propeptides of type 1 collagen: (C-terminal: P1CP, N-terminal: P1NP) 등이 주로 사용되며, 골흡수표지자의 경우 telopeptides of type 1 collagen (C-terminal: CTX-1, N-terminal: NTX-1), hydroxyproline, pyridinium crosslinks (pyridinoline (PYD), deoxypyridinoline (DPD)) 등이 주로 사용된다[ 64- 67]. 골밀도는 20-30대에 최대에 도달하며, 이후로는 점진적인 감소가 이루어진다[ 68]. 골밀도의 감소는 신체활동의 감소, 호르몬 변화, 전염증성 사이토카인의 증가로 인해 유도될 수 있으며, 골다공증과 같이 골밀도가 현저하게 저하된 경우에는 일상적인 활동 중에도 뼈가 부러지는 골다공증성 골절을 경험할 수 있기 때문에 노년기에 적절한 수준의 골밀도를 유지하는 것은 매우 중요하다[ 69]. 혈류제한 운동이 노인들의 골밀도 및 골표지자에 미치는 효과에 관한 선행연구를 종합한 내용은 Table 2에 제시하였다. Karabulut et al. [ 70]의 연구에 따르면 6주간의 혈류제한 저강도 저항성 운동은 골밀도의 유의한 변화를 유도하지 못했지만, 골형성표지자인 ALP와 골형성 비율을 나타내는 ALP/CTX의 유의한 증가를 보여주었으며, 이는 고강도 저항성 운동의 효과와 유사한 수준이었다. 또한 Linero et al. [ 48]의 연구에 따르면 12주간의 혈류제한 저강도 저항성 운동은 골밀도의 변화를 유도하지 못했지만 골형성표지자인 P1NP의 유의한 증가가 나타나는 유사한 결과가 보고되었다. Park et al. [ 71]의 연구에서는 12주간의 혈류제한 저강도 저항성 운동을 통한 골밀도의 증가가 보고되었으며, 골형성표지자인 ALP의 유의한 증가도 함께 나타났다.
Table 2.
Effects of low intensity exercise with blood flow restriction on bone mineral density and bone turnover markers
|
Author |
Subjects |
Group |
Intervention |
Results |
|
Frequency |
Intensity |
Volume |
Type |
|
Karabulut et al., 2011 [70] |
Old men (n=37, 56.8±0.6 yr) |
CON
LIT+BFR
HIT |
6 wks, 3 times/wk |
1RM 20%
1RM 80% |
3 sets (30/15/15 reps)
3 sets, 8 reps |
Resistance exercise |
BMD ↔
ALP↑
ALP/CTX↑ |
|
Linero et al., 2021 [48] |
Old women (n=26, 50-60 yr) |
CON
LIT
LIT+BFR
HIT |
12 wks, 3 times/wk |
1RM 30%
1RM 60-80% |
3 sets, 20 reps
3 sets, 8 reps |
Resistance exercise |
BMD ↔
P1NP↑
CTX ↔
P1NP/CTX ↔ |
|
Park S et al., 2019 [71] |
Old women (n=27, ≥65 yr) |
LIT
LIT+BFR
HIT |
12 wks, 3 times/wk |
1RM 20%
1RM 70% |
3 sets (25/20/15 reps)3
sets, 8 reps |
Resistance exercise |
BMD↑
ALP ↔
CTX ↔ |
일반적으로 골밀도의 증가를 위해서는 높은 하중이나 기계적인 스트레스가 반복되어야 한다[ 72, 73]. 골조직에 물리적인 압력이 가해지는 경우 골내부의 압력이 증가되며, 압력차에 의한 골간질액(bone interstitial fluid)의 흐름이 유도된다[ 74]. 골간질액의 흐름은 전단응력(shear stress)을 발생시켜 골세포를 자극하고 골형성을 유도할 수 있다[ 75, 76]. 혈류제한 운동의 경우 비교적 낮은 운동 강도로 이루어지기 때문에 물리적인 압력보다는 압력 커프를 통한 정맥 폐색으로 골조직의 내압 증가를 일으키며, 간질액의 흐름을 유도할 수 있다고 보고되었다[ 77]. 또한 혈류제한 운동은 압력 커프를 통한 혈류제한을 통해 국소적인 저산소, 허혈 상태를 유발시켜 저산소증 유도 인자 1α (hypoxia-induc-ible factor 1-alpha, HIF-1α)의 발현을 증가시킬 수 있으며[ 78], HIF-1α는 혈관내피세포 성장인자(vascular endothelial growth factor, VEGF)와 같은 혈관신생인자의 전사(transcription)를 촉진한다[ 79]. 실제로 혈류제한 운동을 통해 HIF-1α와 혈관신생인자들의 mRNA의 발현이 증가되었다는 연구결과가 보고되고 있으며[ 80], 혈관신생인자의 발현은 혈관신생과 함께 골조직으로의 혈류를 개선하여 골밀도에 긍정적인 영향을 미칠 수 있다[ 81]. 이외에도 골형성 및 성장에 중요한 성호르몬, GH, IGF-1의 발현이 혈류제한 운동 후 증가했다는 연구결과도 보고되었다[ 55, 56]. 본 종설에서 분석에 포함된 연구들은 모두 골표지자의 긍정적인 변화가 나타났지만 골밀도는 Park et al. [ 71]의 연구에서만 유의미한 변화가 나타났다. 이는 골 리모델링 주기(bone remodeling cycle)가 흡수단계(resorption phase), 역전단계(reversal phase), 형성단계(formation phase)로 구성되며[ 82], 대략 4-6개월 정도가 소요된다는 것을 감안했을 때[ 83- 85] 문헌 분석에 포함된 연구들은 골밀도의 변화를 살펴보기엔 연구기간이 다소 짧았을 수 있으며, 추후 연구에서는 골밀도의 변화를 관찰하기 위해 4개월 이상의 연구가 필요할 것으로 사료된다.
3) 혈류제한 운동의 심혈관 기능에 대한 효과
노화는 심장과 혈관의 구조적, 기능적 변화를 야기한다. 나이가 증가함에 따라 혈관벽은 비후(thickening)되고 경직(stiffening)되며[ 86], 혈관내피세포(vascular endothelial cell) 기능에도 장애가 나타나게 된다[ 87]. 혈관벽의 경직과 내피세포의 기능 장애는 혈관의 확장(vasorelaxation) 능력을 손상시키며, 이러한 변화는 후부하(after load)를 증가시켜 심근 수축 시 심실의 부담 증가와 함께 심실의 병적 비대(patho-logic hypertrophy)를 유발한다[ 88, 89]. 심실 비대는 심실의 섬유화를 동반하며, 심실의 이완능력을 손상시킨다[ 90]. 실제로 Parikh et al. [ 91]의 횡단연구에 따르면 연령 증가에 따라 혈관 경직도(vascular stiffness)의 증가로 인한 후부하 증가가 나타났으며, 좌심실의 확장 능력(left ventricular diastolic function) 및 심박출량(cardiac output)의 감소가 함께 나타났다. 이와 같이 노화에 따른 심혈관계의 구조적, 기능적 변화는 동맥경화증, 고혈압, 심근경색, 심부전 등 심혈관계 질환의 발병 증가로 이어질 수 있다[ 92- 94]. 혈류제한 운동이 노인들의 심혈관 기능에 미치는 효과에 관한 선행연구를 종합한 내용은 Table 3에 제시하였다. 일회성 혈류제한 운동은 동일한 강도의 운동에 비해 운동 중 더 높은 심박수를 유발하였으며, 운동 직후 심박수, 수축기 혈압 및 이완기 혈압의 증가를 유도하였다[ 27, 95- 100]. 이는 혈류제한 운동 시 대사산물의 축적이 골격근의 화학수용체(chemoreceptor)를 자극하고 근육의 대사 반사(muscle metabore-flex) 작용을 유발하여 교감신경계를 활성화시켰거나[ 101, 102], 혈류제한 운동 후 증가된 노르에피네프린(norepinephrine)으로 인한 일시적인 말초혈관의 수축이 유도되었기 때문으로 사료된다[ 102, 103]. 하지만 장기적인 혈류제한 운동의 경우 심박수와 혈압에 부정적인 영향을 주지 않았으며, 오히려 수축기 혈압 및 이완기 혈압의 감소와[ 104, 105] 혈관내피세포 기능 개선[ 98], 동맥순응도(arterial compliance)의 증가가 나타났다[ 52]. 이는 제한됐던 혈류의 재관류 과정에서 전단응력의 증가로 인해 산화질소(nitric oxide, NO)와 같은 내피의존성 혈관확장(endotheli-al-dependent vasorelaxation) 물질의 방출 증가 때문일 것으로 사료된다[ 106]. 또한 혈류제한 운동을 통해 유발될 수 있는 국소적인 허혈 및 저산소 환경은 HIF-1α 발현 증가를 통한 VEGF의 수준을 증가시킨다[ 56, 98]. VEGF는 phospholipase C-Ca 2+/calmodulin (PLC-Ca 2+/CaM) 신호전달 경로를 통해 혈관내피세포기능을 조절하는 내피세포 산화질소 합성효소(endothelial nitric oxide synthase, eNOS)를 활성화시켜 혈관기능에 긍정적인 효과를 줄 수 있다[ 107].
Table 3.
Effects of low intensity exercise with blood flow restriction on cardiovascular function
|
Author |
Subjects |
Group |
Intervention |
Results |
|
Frequency |
Intensity |
Volume |
Type |
|
Ferreira Junior et al., 2019 [104] |
Old men (n=21, 52.4 yr) |
Walk
Walk+BFR |
6 wks, 3 times/wk |
6 km/hr, 5% grade |
5 sets (each set 3 min) |
Walk |
SDNN↑ RMSSD↑, SBP↓, DBP ↔ |
|
Lopes et al., 2021 [105] |
Old adults (n=32, 72±7 yr) |
LIT
LIT+BFR
HIT |
12 wks, 3 times/wk |
1RM 30%
1RM 70% |
3 sets, 10 reps |
Resistance exercise |
SBP↓, DBP↓, MAP↓ |
|
Ozaki et al., 2011a [52] |
Old adults (n=23, 57-76 yr) |
Walk
Walk+BFR |
10 wks, 4 times/wk |
HRR 45% |
20 min |
Walk |
CAC↑, HR ↔, SBP ↔, DBP ↔, MAP ↔ |
|
Parkington et al., 2022 [100] |
Old women (n=10, 64.3±4.2 yr) |
LIT
LIT+BFR
HIT |
Acute |
1RM 20%
1RM 60% |
3-4 sets, 15 reps
4 sets, 10 reps |
Resistance exercise |
HR peak↑, BP ↔, MAP ↔ |
|
Pinto et al., 2016 [27] |
Old women (n=12, 57±7 yr) |
LIT
LIT+BFR
HIT |
Acute |
1RM 20%
1RM 65% |
3 sets, 15 reps
3 sets, 8 reps |
Resistance exercise |
HR↑, SBP↑, DBP↑, SVR↑ |
|
Pinto et al., 2018 [96] |
Old women (n=18, 67±1.7 yr) |
BFR
LIT+BFR
HIT |
Acute |
1RM 20%
1RM 65% |
4 min
3 sets, 10 reps |
Resistance exercise |
SBP↑, DBP↑, SVR↑, CO↓, SV↓ |
|
Sardeli et al., 2017 [97] |
Old adults (n=21, 64.3 yr) |
CON
LIT
LIT+BFR
HIT |
Acute |
1RM 30%
1RM 80% |
4 sets, until failure
4 sets (30/15/15/15 reps)
4 sets, until failure |
Resistance exercise |
SBP↑, DBP↑, MBP↑, TPR ↔, CAC ↔ |
|
Shimizu et al., 2016 [98] |
Old adults (n=40, 71±4 yr) |
LIT
LIT+BFR |
Acute |
1RM 20% |
3 sets, 20 reps |
Resistance exercise |
HR↑, SBP↑, DBP↑ |
|
Shimizu et al., 2016 [98] |
Old adults (n=40, 71±4 yr) |
LIT
LIT+BFR |
4 wks, 3 times/wk |
1RM 20% |
3 sets, 20 reps |
Resistance exercise |
RHI↑, vWF↓ |
|
Staunton et al., 2015 [95] |
Old men (n=13, 70±5 yr) |
AT
AT+BFR |
Acute |
4 km/hr (AT) |
4 sets (each set 2 min) |
Walk |
HR↑, SBP↑, MAP↑, CO ↔ |
|
Staunton et al., 2015 [95] |
Old men (n=13, 70±5 yr) |
LIT
LIT+BFR |
Acute |
1RM 20% (RT) |
4 sets (30/15/15/15 reps) |
Resistance exercise |
HR↑, SBP↑, MAP↑, CO ↔ |
|
Vieira et al., 2013 [99] |
Old men (n=12, 66±7 yr) |
LIT
LIT+BFR |
Acute |
1RM 30% |
3 min |
Resistance exercise |
HR↑, SBP↑, DBP↑, MBP↑, CVR↑, CBF↓ |
4) 혈류제한 운동의 인지기능에 대한 효과
뇌의 크기는 노화에 따라 감소하게 되며[ 108], 특히 해마(hippocam-pus)를 포함하는 측두엽(temporal lobe)과 전두엽(frontal lobe)에서 가장 큰 감소가 나타난다[ 109, 110]. 노화와 관련된 뇌의 부피 감소는 신경세포 사멸 및 수상돌기(dendrite)와 축삭(axon)의 감소로 인한 시냅스(synapse) 손실 등이 원인으로 알려져 있으며[ 111], 이러한 뇌의 구조적인 변화는 인지기능 저하와 같은 뇌 기능의 변화를 야기한다[ 112]. 인지기능이란 주의력, 기억력, 문제해결능력 등을 포함한 다양한 정신적인 과정으로 일상생활을 영위하는데 매우 중요한 능력이다[ 113]. 노화로 인한 인지기능 저하를 예방하거나 개선하기 위한 효과적인 중재 방법 중 하나는 운동으로 알려져 있으며, 실제로 많은 연구들을 통해 인지기능에 대한 운동의 효과가 검증되었다[ 10, 114]. 하지만 혈류제한 운동과 인지기능에 관한 연구는 매우 제한적이며, 본 종설에서는 단 2개의 연구만이 자료분석에 포함되었다. 혈류제한 운동이 노인들의 인지기능에 미치는 효과에 관한 선행연구를 종합한 내용은 Table 4에 요약하여 제시하였다. Sardeli et al. [ 115]의 연구에 따르면 일회성 혈류제한 저항성 운동은 인지기능 평가 도구 인 Stroop color and word task의 정답률과 반응시간에 유의한 변화를 나타내지 않았다. 또한 Kargaran et al. [ 51]의 연구에 따르면 인지과제와 저강도 유산소 운동을 결합한 이중과제(dual-task) 운동을 혈류제한과 함께 8주간 실시한 결과, 인지기능 평가 도구인 mini-mental state examination (MMSE)의 점수에 유의한 변화는 나타나지 않았지만 신경영양인자(neurotrophic factor)로 알려진 뇌유래신경영양인자(brain-derived neurotrophic factor, BDNF)의 발현은 유의하게 증가하였다.
Table 4.
Effects of low intensity exercise with blood flow restriction on cognitive function
|
Author |
Subjects |
Group |
Intervention |
Results |
|
Frequency |
Intensity |
Volume |
Type |
|
Kargaran et al., 2021 [51] |
Old women (n=24, 62.9±3.1 yr) |
CON
DT
DT+BFR |
8 wks, 3 times/wk |
HRR 45% |
20 min |
Walk+CT |
MMSE ↔ BDNF↑ |
|
Sardeli et al., 2018 [115] |
Old adults (n=21, 64.3±5.04 yr) |
CON
LIRT
LIRT+BFR
HIRT |
Acute |
1RM 30%
1RM 80% |
4 sets, until failure
4 sets (30/15/15/15 reps)
4 sets, until failure |
Resistance exercise |
Stroop task Reaction time ↔ Accuracy ↔ |
혈류제한 운동 시, 혈류제한으로 인한 속근 섬유의 동원 증가와 젖산 제거율의 감소로 젖산 축적이 증가된다[ 116, 117]. 혈중 젖산 농도의 증가는 대뇌의 젖산 흡수를 증가시킬 수 있으며, 이는 젖산이 모노카르복실레이트 수송체(monocarboxylate transporters, MCTs)에 의해 뇌혈관장벽(brain-blood barrier, BBB)을 통과할 수 있기 때문이다[ 118]. 젖산은 뇌에서 직접적인 에너지원으로 사용될 수 있을 뿐만 아니라[ 119, 120], 신경 세포의 성장과 생존, 학습 및 기억에 중요한 역할을 하는 BDNF의 발현을 증가시키고 인지기능을 향상시킬 수 있다[ 121, 122]. 또한 젖산은 IGF-1, VEGF와 같이 신경보호효과가 있는 호르몬의 발현 증가와 관련이 있으며[ 123], 뇌 혈관에서 젖산염 수용체(hydroxycarboxylic acid receptor 1, HCAR1)를 통해서 뇌혈관신생을 촉진시킬 수 있다[ 124]. 실제로 혈류제한 운동 후 뇌혈류 증가 및 대뇌 피질의 활성화 증가가 유도되었다는 연구 결과가 보고되고 있다[ 125, 126]. 종합해보면 혈류제한 운동이 인지기능에 효과적인 운동 방법이 될 수 있는 가능성이 제시되고 있지만 본 종설에 포함된 연구에서 혈류제한 운동은 BDNF의 증가를 유도하였을 뿐, 인지기능 개선에 유의미한 효과를 나타내지 못했다. 이러한 결과는 혈류제한 저강도 유산소 운동이 젊은 성인 남성의 인지기능 개선에 효과적이라고 보고한 Sugimoto et al. [ 127]의 연구와는 상충되는 결과다. 이는 혈류제한 운동과 인지기능에 관한 연구가 매우 제한적이며, 연구마다 운동 중재 및 인지기능 평가 방법이 다르기 때문인 것으로 사료된다. 향후 인지기능과 혈류제한 운동에 관한 추가적인 연구가 필요하다.
2. 혈류제한 운동의 안전성과 적용 가능성
혈류제한 운동은 압력 커프의 착용으로 인해 혈류제한 부위에 국소적인 불편감과 근육통이 유발될 수 있으며, 혈압 증가와 함께 혈전증(thrombosis) 및 횡문근융해증(rhabdomyolysis)과 같은 부작용을 야기할 수 있다는 우려가 제기되어 왔다[ 128]. 따라서, 심혈관계 질환을 앓고 있거나 관련 질환의 병력을 가지고 있는 경우 혈류제한 운동은 권장되지 않았다[ 128]. 하지만 최근 메타분석 연구에 따르면 고혈압을 가지고 있는 노인들에게 혈류제한 운동의 부작용이 확인되지 않았으며[ 129], 혈류제한 운동이 고혈압이나 관상동맥질환(coronary artery disease)을 가지고 있는 노인들의 혈압을 개선시키는 결과가 보고되면서 혈류제한 운동의 안전성이 확인되고 있다[ 130, 131]. 드물게 혈류제한 운동을 통해 혈전증, 횡문근융해증과 같은 부작용이 보고된 바 있으나, 이러한 부작용은 동맥 폐색을 유발할 수 있는 과도한 커프 압력, 장시간의 혈류제한이 원인으로 사료되며[ 132, 133], Nakajima et al. [ 134]의 연구에 따르면 혈전증, 횡문근융해증과 같은 혈류제한 운동의 부작용 발생 빈도는 0.055%와 0.008%에 해당할 정도로 매우 낮은 수준이었다. 이처럼 혈류제한 운동은 노인들의 심혈관계 질환의 위험성을 증가시키지 않으며 부작용 발생 위험 또한 매우 낮은 수준으로 판단되지만 관련 연구가 부족한 실정이다. 따라서 노인들에게 혈류제한 운동을 적용할 경우, 혈류제한 운동으로 유발될 수 있는 불편감 및 잠재적인 위험성을 최소화하고, 안전성을 높이기 위해서 적절한 압력 및 압박 시간, 커프의 너비 및 재질 등을 고려하는 것이 적절하다[ 135]. 혈류제한은 정맥의 흐름을 제한하는 것이 목적이며, 동맥의 흐름을 완전히 차단하지 않을 정도의 적절한 압력을 사용하는 것이 바람직하다[ 136]. 따라서 커프 압력은 동맥폐색압력(arterial occlusion pressure, AOP), 사지폐색압력(limb occlusion pressure, LOP), 수축기 혈압과 같은 압력의 백분율(%)로 개별적인 압력 설정을 하는 것이 적절하다[ 137, 138]. 또한 동일한 압력일지라도 커프 너비에 따라 혈관 폐색 정도가 다르기 때문에 커프의 너비나 재질과 같은 요소도 고려해야 한다[ 137]. 이외에도 장시간의 혈류제한 시간은 조직 괴사 및 신경계 손상 등 부정적인 영향을 미칠 수 있기 때문에 혈류제한의 적용시간은 상지(upper limb)의 경우 최대 15분, 하지(lower limb)의 경우 최대 20분을 초과하지 않는 것이 적절하다[ 139]. 종합해보면 노인들에게 혈류제한 운동의 위험성을 명확히 입증할 수 있는 연구는 아직 보고된 바 없으며, 부작용의 발생 위험 또한 매우 낮은 것으로 판단된다. 하지만 관련 연구가 아직 충분하지 않은 실정이고, 운동이 익숙하지 않은 노인에게 혈류제한 운동을 실시할 경우 다양한 요소(커프 압력, 압박 시간, 커프 너비 및 재질)를 고려하여 운동 중재를 해야 되기 때문에 임상이나 현장에서 쉽게 적용되기에는 일부 제한점이 존재한다. 이러한 점을 고려해서 노인들에게 혈류제한 운동 중재 시에는 혈류제한 운동에 관해 적절한 교육을 받은 전문가와 함께 혈류제한 운동의 다양한 요소를 고려하여 잠재적 위험성을 최소화하고 안전성을 높이는 것이 적절할 것으로 사료된다. 또한 안정성을 확보하면서 동시에 운동 효과를 극대화하기 위해서는 노인들에게 적합한 혈류제한 운동 방법에 대해 구체적인 권장사항에 관한 향후 추가적인 연구가 필요하다.
결 론
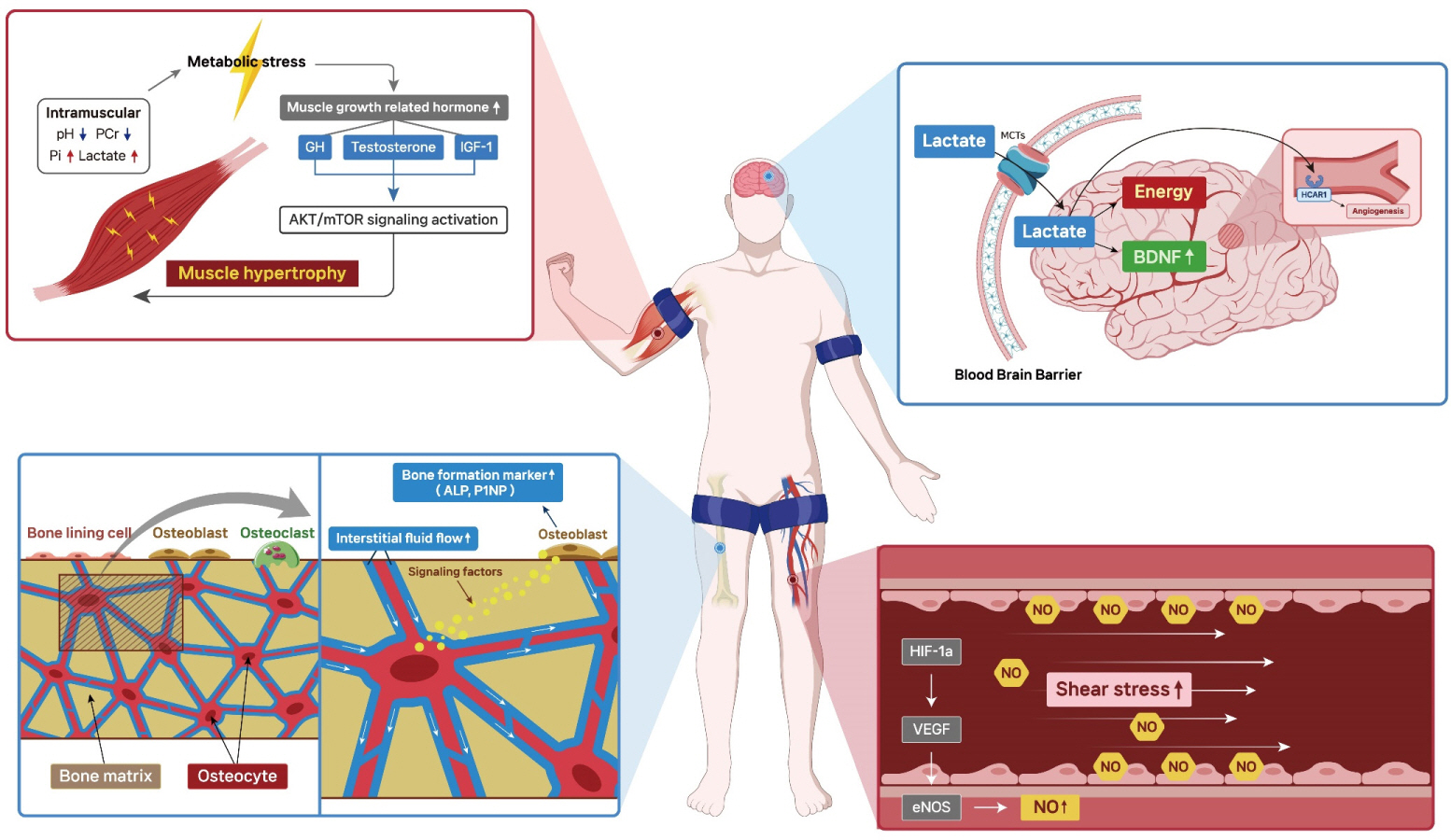
본 종설에서는 혈류제한 운동이 노인들의 골격근 및 근력, 골밀도, 심혈관 기능, 인지기능에 미치는 영향에 관한 선행 연구들을 종합, 분석하여 성공적인 노화를 위한 효과적인 운동 중재 방법으로 혈류제한 운동의 효과를 검토하고 적용 가능성을 고찰하였다. 혈류제한 운동의 잠재적인 효과와 관련기전에 관해 정리한 내용은 Fig. 1에 요약하여 제시하였다. 혈류제한 운동은 노인들의 골격근 및 근력 증가에 효과적이며, 장기적인 혈류제한 운동을 통해서는 혈압 감소, 내피세포 기능 향상, 동맥순응도 향상 등의 효과가 나타났다. 골밀도와 인지기능에 관해서는 연구가 매우 제한적이며, 연구마다 결과가 상이하기 때문에 혈류제한 운동이 골밀도와 인지기능에 미치는 영향에 대해서는 아직 불분명한 실정이다. 하지만 혈류제한 운동이 노인들의 골표지자의 긍정적인 변화를 유도하고 신경영양인자의 발현을 증가시킨 것으로 보았을 때, 혈류제한 운동은 노인들의 골밀도 및 인지기능에도 긍정적인 효과를 보일 수 있을 것으로 사료되며, 향후 추가적인 연구가 필요하다. 혈류제한 운동은 커프 압력, 압박 시간, 커프 너비 및 재질 등의 요소를 고려하여 진행될 때, 노인들의 성공적인 노화를 위한 효과적이고 안전한 운동 중재 방법으로 활용될 수 있을 것이라 판단된다.
Fig. 1.
Fig. 1.
Potential pleiotropic effects of blood flow restriction exercise on successful aging.
BFRE promotes muscle hypertrophy by increasing metabolic stress and muscle growth-related hormones. BFRE can also increase bone formation markers such as ALP and P1NP which are induced via increased bone interstitial fluid flow. BFRE-induced local ischemic/hypoxic environment in skeletal muscle enhances vascular endothelial function by increasing HIF-1α expression and VEGF stimulating NO synthesis. In addition, ischemia-reperfusion cycles during BFRE may increase shear stress stimulating vascular endothelial cells and increasing NO production. Increased lactate by BFRE can cross the blood brain barrier and be used as an energy source for the brain as well as stimulating BDNF. Additionally, increased lactate promotes angiogenesis in cerebral vessels via the lactate receptor HCAR1.
AKT, protein kinase B; ALP, alkaline phosphatase; BDNF, brain-derived neurotrophic factor; BFRE, blood flow restriction exercise; eNOS, endothelial nitric oxide synthase; GH, growth hormone; HCAR1, hydroxycarboxylic acid receptor 1; HIF-1α, hypoxia-inducible factor 1-alpha; IGF-1, insulin-like growth fac-tor-1; MCTs, monocarboxylate transporters; mTOR, mammalian target of rapamycin; NO, nitric oxide; P1NP, Procollagen type 1 N-terminal Propeptide; PCr, phosphocreatine; Pi, inorganic phosphate; VEGF, vascular endothelial growth factor.
REFERENCES
1. Brown GC. Living too long: the current focus of medical research on increasing the quantity, rather than the quality, of life is damaging our health and harming the economy. EMBO Rep. 2015;16(2):137-41.  2. de Magalhães JP, Stevens M, Thornton D. The Business of Anti-Aging Science. Trends Biotechnol. 2017;35(11):1062-73.  5. WHO. A, WHO Methods and Data Sources for Life Tables 1990-2019. 2020;World Health Organization Geneva.
7. Urtamo A, Jyväkorpi SK, Strandberg TE. Definitions of successful ageing: a brief review of a multidimensional concept. Acta Biomed. 2019;90(2):359-63.  8. Leung FP, Yung LM, Laher I, Yao X, Chen ZY, et al. Exercise, vascular wall and cardiovascular diseases: an update (Part 1). Sports Med. 2008;38(12):1009-24. 9. Yung LM, Laher I, Yao X, Chen ZY, Huang Y, et al. Exercise, vascular wall and cardiovascular diseases: an update (part 2). Sports Med. 2009;39(1):45-63.
11. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25(Suppl 3):1-72. 13. Franklin BA, Thompson PD, Al-Zaiti SS, Albert CM, Hivert MF, et al. Exercise-related acute cardiovascular events and potential deleteri-ous adaptations following long-term exercise training: placing the risks into perspective-an update: a scientific statement from the amer-ican heart association. Circulation. 2020;141(13):e705-36. 14. Medicine ACoS, Thompson PD, Franklin BA, Balady GJ, Blair SN, et al. Exercise and acute cardiovascular events: placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358-68. 15. Liu CJ, Latham N. Adverse events reported in progressive resistance strength training trials in older adults: 2 sides of a coin. Arch Phys Med Rehabil. 2010;91(9):1471-3. 16. Kim J, Lang JA, Pilania N, Franke WD. Effects of blood flow restricted exercise training on muscular strength and blood flow in older adults. Exp Gerontol. 2017;99:127-32. 17. Pope ZK, Willardson JM, Schoenfeld BJ. Exercise and blood flow restriction. The Journal of Strength & Conditioning Research. 2013;27(10):2914-26. 20. Takada S, Okita K, Suga T, Omokawa M, Kadoguchi T, et al. Low-in-tensity exercise can increase muscle mass and strength proportionally to enhanced metabolic stress under ischemic conditions. J Appl Physiol. (1985). 2012;113(2):199-205.
21. Suga T, Okita K, Morita N, Yokota T, Hirabayashi K, et al. Intramus-cular metabolism during low-intensity resistance exercise with blood flow restriction. J Appl Physiol. (1985). 2009;106(4):1119-24.
22. Suga T, Okita K, Morita N, Yokota T, Hirabayashi K, et al. Dose effect on intramuscular metabolic stress during low-intensity resistance exercise with blood flow restriction. J Appl Physiol. (1985). 2010;108(6):1563-7.
23. Sugaya M, Yasuda T, Suga T, Okita K, Abe T. Change in intramuscular inorganic phosphate during multiple sets of blood flow-restricted low-intensity exercise. Clin Physiol Funct Imaging. 2011;31(5):411-3. 24. Rodrigues R, Ferraz RB, Kurimori CO, Guedes LK, Lima FR, et al. Low-load resistance training with blood-flow restriction in relation to muscle function, mass, and functionality in women with rheuma-toid arthritis. Arthritis Care Res. (Hoboken). 2020;72(6):787-97.
25. Ferraz RB, Gualano B, Rodrigues R, Kurimori CO, Fuller R, et al. Benefits of resistance training with blood flow restriction in knee os-teoarthritis. Med Sci Sports Exerc. 2018;50(5):897-905. 26. Hughes L, Rosenblatt B, Haddad F, Gissane C, McCarthy D, et al. Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of an-terior cruciate ligament reconstruction patients: A UK National Health Service Randomised Controlled Trial. Sports Med. 2019;49(11):1787-805.  27. Pinto RR, Polito MD. Haemodynamic responses during resistance exercise with blood flow restriction in hypertensive subjects. Clin Physiol Funct Imaging. 2016;36(5):407-13. 28. Franklin SS, Gustin WT, Wong ND, Larson MG, Weber MA, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation. 1997;96(1):308-15. 29. Berger C, Langsetmo L, Joseph L, Hanley DA, Davison KS, et al. Change in bone mineral density as a function of age in women and men and association with the use of antiresorptive agents. Cmaj. 2008;178(13):1660-8. 30. Proctor D, Balagopal P, Nair K. Age-related sarcopenia in humans is associated with reduced synthetic rates of specific muscle proteins. The Journal of nutrition. 1998;128(2):351S-5S. 31. Volpi E, Nazemi R, Fujita S. Muscle tissue changes with aging. Curr Opin Clin Nutr Metab Care. 2004;7(4):405-10. 32. Hughes VA, Frontera WR, Roubenoff R, Evans WJ, Singh MA. Longitudinal changes in body composition in older men and women: role of body weight change and physical activity. Am J Clin Nutr. 2002;76(2):473-81. 33. Thomas DR. Loss of skeletal muscle mass in aging: examining the relationship of starvation, sarcopenia and cachexia. Clin Nutr. 2007;26(4):389-99. 34. Fry CS, Drummond MJ, Glynn EL, Dickinson JM, Gundermann DM, et al. Aging impairs contraction-induced human skeletal muscle mTORC1 signaling and protein synthesis. Skelet Muscle. 2011;1(1):11. 35. Delmonico MJ, Harris TB, Visser M, Park SW, Conroy MB, et al. Longitudinal study of muscle strength, quality, and adipose tissue in-filtration. Am J Clin Nutr. 2009;90(6):1579-85. 36. Marzetti E, Calvani R, Tosato M, Cesari M, Di Bari M, et al. Sarcopenia: an overview. Aging Clin Exp Res. 2017;29(1):11-7. 37. Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, et al. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc. 2007;55(5):769-74. 38. Landi F, Liperoti R, Russo A, Giovannini S, Tosato M, et al. Sarcopenia as a risk factor for falls in elderly individuals: results from the il-SIRENTE study. Clin Nutr. 2012;31(5):652-8. 39. He N, Zhang Y, Zhang L, Zhang S, Ye H. Relationship between sarcopenia and cardiovascular diseases in the elderly: An Overview. Front Cardiovasc Med. 2021;8:743710. 40. Brown JC, Harhay MO, Harhay MN. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J Ca-chexia Sarcopenia Muscle. 2016;7(3):290-8. 41. Pacifico J, Geerlings MAJ, Reijnierse EM, Phassouliotis C, Lim WK, et al. Prevalence of sarcopenia as a comorbid disease: a systematic review and meta-analysis. Exp Gerontol. 2020;131:110801. 42. Silva M, Pereira P, Geraldes A. Effects of resistance training with blood flow restriction on the body composition of postmenopausal women. Int Phys Med Rehab J. 2018;3(3):195-8.
43. Letieri RV, Teixeira AM, Furtado GE, Lamboglia CG, Rees JL, et al. Effect of 16 weeks of resistance exercise and detraining comparing two methods of blood flow restriction in muscle strength of healthy older women: a randomized controlled trial. Exp Gerontol. 2018;114:78-86. 44. Libardi CA, Chacon-Mikahil MP, Cavaglieri CR, Tricoli V, Roschel H, et al. Effect of concurrent training with blood flow restriction in the elderly. Int J Sports Med. 2015;36(5):395-9. 45. Cook SB, LaRoche DP, Villa MR, Barile H, Manini TM. Blood flow restricted resistance training in older adults at risk of mobility limitations. Exp Gerontol. 2017;99:138-45. 46. Vechin FC, Libardi CA, Conceição MS, Damas FR, Lixandrão ME, et al. Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J Strength Cond Res. 2015;29(4):1071-6. 47. Karabulut M, Abe T, Sato Y, Bemben MG. The effects of low-intensi-ty resistance training with vascular restriction on leg muscle strength in older men. Eur J Appl Physiol. 2010;108(1):147-55. 48. Linero C, Choi SJ. Effect of blood flow restriction during low-inten-sity resistance training on bone markers and physical functions in postmenopausal women. J Exerc Sci Fit. 2021;19(1):57-65. 49. Pereira Neto EA, Bittar ST, Silva JCGd, Pfeiffer PAS, Santos HHd, et al. Walking with blood flow restriction improves the dynamic strength of women with osteoporosis. Revista Brasileira de Medicina do Esporte. 2018;24:135-9. 50. Abe T, Sakamaki M, Fujita S, Ozaki H, Sugaya M, et al. Effects of low-intensity walk training with restricted leg blood flow on muscle strength and aerobic capacity in older adults. J Geriatr Phys Ther. 2010;33(1):34-40. 51. Kargaran A, Abedinpour A, Saadatmehr Z, Yaali R, Amani-Shalamzari S, et al. Effects of dual-task training with blood flow restriction on cognitive functions, muscle quality, and circulatory biomarkers in elderly women. Physiol Behav. 2021;239:113500. 52. Ozaki H, Miyachi M, Nakajima T, Abe T. Effects of 10 weeks walk training with leg blood flow reduction on carotid arterial compliance and muscle size in the elderly adults. Angiology. 2011;62(1):81-6. 53. Ozaki H, Sakamaki M, Yasuda T, Fujita S, Ogasawara R, et al. In-creases in thigh muscle volume and strength by walk training with leg blood flow reduction in older participants. J Gerontol A Biol Sci Med Sci. 2011;66(3):257-63. 54. Takarada Y, Nakamura Y, Aruga S, Onda T, Miyazaki S, et al. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol. (1985). 2000;88(1):61-5.
55. Yinghao L, Jing Y, Yongqi W, Jianming Z, Zeng G, et al. Effects of a blood flow restriction exercise under different pressures on testoster-one, growth hormone, and insulin-like growth factor levels. J Int Med Res. 2021;49(9):3000605211039564. 56. Patterson SD, Leggate M, Nimmo MA, Ferguson RA. Circulating hormone and cytokine response to low-load resistance training with blood flow restriction in older men. Eur J Appl Physiol. 2013;113(3):713-9. 57. Yoon MS. mTOR as a Key Regulator in Maintaining Skeletal Muscle Mass. Front Physiol. 2017;8:788. 58. Fry CS, Glynn EL, Drummond MJ, Timmerman KL, Fujita S, et al. Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men. J Appl Physiol. (1985). 2010;108(5):1199-209. 59. Sundberg CJ. Exercise and training during graded leg ischaemia in healthy man with special reference to effects on skeletal muscle. Acta Physiol Scand Suppl. 1994;615:1-50. 60. Nilwik R, Snijders T, Leenders M, Groen BB, van Kranenburg J, et al. The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Exp Gerontol. 2013;48(5):492-8. 61. Lexell J. Human aging, muscle mass, and fiber type composition. J Gerontol A Biol Sci Med Sci. 1995;50:Spec No: 11-6..
62. Ladlow P, Coppack RJ, Dharm-Datta S, Conway D, Sellon E, et al. Low-load resistance training with blood flow restriction improves clinical outcomes in musculoskeletal rehabilitation: A Single-Blind Randomized Controlled Trial. Front Physiol. 2018;9:1269. 63. Mora S, Bachrach L, Gilsanz V. Noninvasive techniques for bone mass measurement, in Pediatric Bone: Biology & Diseases. Elsevier Inc. 2003;(pp. 303-24).
64. Friedman AW. Important determinants of bone strength: beyond bone mineral density. J Clin Rheumatol. 2006;12(2):70-7. 65. Shetty S, Kapoor N, Bondu JD, Thomas N, Paul TV. Bone turnover markers: Emerging tool in the management of osteoporosis. Indian J Endocrinol Metab. 2016;20(6):846-52. 66. Vincent KR, Braith RW. Resistance exercise and bone turnover in elderly men and women. Med Sci Sports Exerc. 2002;34(1):17-23. 67. Woitge HW, Friedmann B, Suttner S, Farahmand I, Müller M, et al. Changes in bone turnover induced by aerobic and anaerobic exercise in young males. J Bone Miner Res. 1998;13(12):1797-804. 68. Melton LJ 3rd, Khosla S, Atkinson EJ, Oconnor MK, Ofallon WM, et al. Cross-sectional versus longitudinal evaluation of bone loss in men and women. Osteoporos Int. 2000;11(7):592-9. 69. Leslie WD, Tsang JF, Caetano PA, Lix LM. Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab. 2007;92(1):77-81. 70. Karabulut M, Bemben DA, Sherk VD, Anderson MA, Abe T, et al. Effects of high-intensity resistance training and low-intensity resistance training with vascular restriction on bone markers in older men. Eur J Appl Physiol. 2011;111(8):1659-67. 71. Park SB, Lee JS, Ahn JY, Son WK, Yoon SJ. Effect of low-intensity re-sistance training with blood flow restriction on serum VEGF level, bone markers and bone mineral density in elderly women. Korean Journal of Sport Science. 2019;30(3):459-69. 72. Chen JH, Liu C, You L, Simmons CA. Boning up on Wolff's Law: mechanical regulation of the cells that make and maintain bone. Journal of biomechanics. 2010;43(1):108-18. 73. Sundh D, Nilsson M, Zoulakis M, Pasco C, Yilmaz M, et al. High-Impact mechanical loading increases bone material strength in postmenopausal women-a 3-month intervention study. J Bone Miner Res. 2018;33(7):1242-51. 74. Price C, Zhou X, Li W, Wang L. Real-time measurement of solute transport within the lacunar-canalicular system of mechanically loaded bone: direct evidence for load-induced fluid flow. J Bone Miner Res. 2011;26(2):277285. 75. Chen JH, Liu C, You L, Simmons CA. Boning up on Wolff's Law: mechanical regulation of the cells that make and maintain bone. J Biomech. 2010;43(1):108-18. 76. Loenneke JP, Young KC, Fahs CA, Rossow LM, Bemben DA, et al. Blood flow restriction: rationale for improving bone. Med Hypothe-ses. 2012;78(4):523-7. 77. Bergula AP, Huang W, Frangos JA. Femoral vein ligation increases bone mass in the hindlimb suspended rat. Bone. 1999;24(3):171-7. 78. Larkin KA, Macneil RG, Dirain M, Sandesara B, Manini TM, et al. Blood flow restriction enhances post-resistance exercise angiogenic gene expression. Med Sci Sports Exerc. 2012;44(11):2077-83. 79. Forsythe JA, Jiang BH, Iyer NV, Agani F, Leung SW, et al. Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol Cell Biol. 1996;16(9):4604-13. 80. Ferguson RA, Hunt JEA, Lewis MP, Martin NRW, Player DJ, et al. The acute angiogenic signalling response to low-load resistance exercise with blood flow restriction. Eur J Sport Sci. 2018;18(3):397-406. 81. Zelzer E, Mamluk R, Ferrara N, Johnson RS, Schipani E, et al. VEG-FA is necessary for chondrocyte survival during bone development. Development. 2004;131(9):2161-71. 82. Hadjidakis DJ, Androulakis II. Bone remodeling. Ann N Y Acad Sci. 2006;1092:385-96. 83. Eriksen EF, Melsen F, Mosekilde L. Reconstruction of the resorptive site in iliac trabecular bone: a kinetic model for bone resorption in 20 normal individuals. Metab Bone Dis Relat Res. 1984;5(5):235-42. 84. Eriksen EF, Gundersen HJ, Melsen F, Mosekilde L. Reconstruction of the formative site in iliac trabecular bone in 20 normal individuals employing a kinetic model for matrix and mineral apposition. Metab Bone Dis Relat Res. 1984;5(5):243-52. 85. Agerbaek MO, Eriksen EF, Kragstrup J, Mosekilde L, Melsen F. A reconstruction of the remodelling cycle in normal human cortical iliac bone. Bone Miner. 1991;12(2):101-12. 86. van den Munckhof I, Scholten R, Cable NT, Hopman MT, Green DJ, et al. Impact of age and sex on carotid and peripheral arterial wall thickness in humans. Acta Physiol (Oxf). 2012;206(4):220-8. 87. Brandes RP, Fleming I, Busse R. Endothelial aging. Cardiovasc Res. 2005;66(2):286-94. 88. Hirt MN, Sörensen NA, Bartholdt LM, Boeddinghaus J, Schaaf S, et al. Increased afterload induces pathological cardiac hypertrophy: a new in vitro model. Basic Res Cardiol. 2012;107(6):307. 89. Ohyama Y, Ambale-Venkatesh B, Noda C, Chugh AR, Teixido-Tura G, et al. Association of aortic stiffness with left ventricular remodeling and reduced left ventricular function measured by magnetic resonance imaging: the multi-ethnic study of atherosclerosis. Circ Cardiovasc Imaging. 2016;9(7).
90. Garg P, Assadi H, Jones R, Chan WB, Metherall P, et al. Left ventricular fibrosis and hypertrophy are associated with mortality in heart failure with preserved ejection fraction. Sci Rep. 2021;11(1):617. 91. Parikh JD, Hollingsworth KG, Wallace D, Blamire AM, MacGowan GA. Normal age-related changes in left ventricular function: role of afterload and subendocardial dysfunction. Int J Cardiol. 2016;223:306-12. 92. North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. 2012;110(8):1097-108. 93. Triposkiadis F, Xanthopoulos A, Butler J. Cardiovascular aging and heart failure: JACC Review Topic of the Week. J Am Coll Cardiol. 2019;74(6):804-13. 94. Mehta RH, Rathore SS, Radford MJ, Wang Y, Wang Y, et al. Acute myocardial infarction in the elderly: differences by age. J Am Coll Cardiol. 2001;38(3):736-41. 95. Staunton CA, May AK, Brandner CR, Warmington SA. Haemody-namics of aerobic and resistance blood flow restriction exercise in young and older adults. Eur J Appl Physiol. 2015;115(11):2293-302. 96. Pinto RR, Karabulut M, Poton R, Polito MD. Acute resistance exercise with blood flow restriction in elderly hypertensive women: hae-modynamic, rating of perceived exertion and blood lactate. Clin Physiol Funct Imaging. 2018;38(1):17-24. 97. Sardeli AV, do Carmo Santos L, Ferreira MLV, Gáspari AF, Rodrigues B, et al. Cardiovascular responses to different resistance exercise pro-tocols in elderly. Int J Sports Med. 2017;38(12):928-36. 98. Shimizu R, Hotta K, Yamamoto S, Matsumoto T, Kamiya K, et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur J Appl Physiol. 2016;116(4):749-57. 99. Vieira PJ, Chiappa GR, Umpierre D, Stein R, Ribeiro JP. Hemodynamic responses to resistance exercise with restricted blood flow in young and older men. The Journal of Strength & Conditioning Research. 2013;27(8):2288-94. 100. Parkington T, Maden-Wilkinson T, Klonizakis M, Broom D. Com-parative perceptual, affective, and cardiovascular responses between resistance exercise with and without blood flow restriction in older adults. International Journal of Environmental Research and Public Health. 2022;19(23):16000. 101. Iida H, Takano H, Meguro K, Asada K, Oonuma H, et al. Hemodynamic and autonomic nervous responses to the restriction of femoral blood flow by KAATSU. International Journal of KAATSU Training Research. 2005;1(2):57-64. 102. Iida H, Kurano M, Takano H, Kubota N, Morita T, et al. Hemodynamic and neurohumoral responses to the restriction of femoral blood flow by KAATSU in healthy subjects. Eur J Appl Physiol. 2007;100(3):275-85. 103. Ozaki H, Loenneke JP, Abe T. Blood flow-restricted walking in older women: does the acute hormonal response associate with muscle hypertrophy? Clinical physiology and functional imaging. 2017;37(4):379-83. 104. Ferreira Junior A, Schamne JC, Altimari LR, Okano AH, Okuno NM. Effect of walk training combined with blood flow restriction on resting heart rate variability and resting blood pressure in middle-aged men. Motriz: Revista de Educação Física. 2019;25. 105. Lopes KG, Farinatti P, Bottino DA, MDGC DES, Maranhão PA, et al. Does resistance training with blood flow restriction affect blood pressure and cardiac autonomic modulation in older adults? Int J Exerc Sci. 2021;14(3):410-22. 106. Kimura M, Ueda K, Goto C, Jitsuiki D, Nishioka K, et al. Repetition of ischemic preconditioning augments endothelium-dependent va-sodilation in humans: role of endothelium-derived nitric oxide and endothelial progenitor cells. Arterioscler Thromb Vasc Biol. 2007;27(6):1403-10. 107. Gélinas DS, Bernatchez PN, Rollin S, Bazan NG, Sirois MG. Imme-diate and delayed VEGF-mediated NO synthesis in endothelial cells: role of PI3K, PKC and PLC pathways. Br J Pharmacol. 2002;137(7):1021-30. 108. Scahill RI, Frost C, Jenkins R, Whitwell JL, Rossor MN, et al. A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging. Arch Neurol. 2003;60(7):989-94. 109. Raz N, Lindenberger U, Rodrigue KM, Kennedy KM, Head D, et al. Regional brain changes in aging healthy adults: general trends, indi-vidual differences and modifiers. Cerebral Cortex. 2005;15(11):1676-89. 110. DeCarli C, Massaro J, Harvey D, Hald J, Tullberg M, et al. Measures of brain morphology and infarction in the framingham heart study: establishing what is normal. Neurobiol Aging. 2005;26(4):491-510. 111. Harding A, Halliday G, Kril J. Variation in hippocampal neuron number with age and brain volume. Cerebral cortex. (New York, NY: 1991). 1998;8(8):710-8.
112. Sluimer JD, van der Flier WM, Karas GB, Fox NC, Scheltens P, et al. Whole-brain atrophy rate and cognitive decline: longitudinal MR study of memory clinic patients. Radiology. 2008;248(2):590-8. 113. Fisher GG, Chacon M, Chaffee DS. Theories of cognitive aging and work, in Work across the lifespan. Elsevier 2019;(pp. 17-45).
114. Kramer AF, Erickson KI. Capitalizing on cortical plasticity: influence of physical activity on cognition and brain function. Trends Cogn Sci. 2007;11(8):342-8. 115. Sardeli AV, Ferreira MLV, Santos LdC, Rodrigues MdS, Damasceno A, et al. Low-load resistance exercise improves cognitive function in older adults. Revista Brasileira de Medicina do Esporte. 2018;24:125-9. 116. Lundberg G, Olofsson P, Ungerstedt U, Jansson E, Sundberg CJ. Lactate concentrations in human skeletal muscle biopsy, microdialysate and venous blood during dynamic exercise under blood flow restriction. Pflugers Arch. 2002;443(3):458-65. 117. Takarada Y, Nakamura Y, Aruga S, Onda T, Miyazaki S, et al. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. Journal of applied physiology. 2000;88(1):61-5. 118. Quistorff B, Secher NH, Van Lieshout JJ. Lactate fuels the human brain during exercise. Faseb j. 2008;22(10):3443-9. 119. Bergersen LH. Lactate transport and signaling in the brain: potential therapeutic targets and roles in body-brain interaction. J Cereb Blood Flow Metab. 2015;35(2):176-85. 120. Dienel GA. Brain lactate metabolism: the discoveries and the contro-versies. J Cereb Blood Flow Metab. 2012;32(7):1107-38. 121. El Hayek L, Khalifeh M, Zibara V, Abi Assaad R, Emmanuel N, et al. Lactate mediates the effects of exercise on learning and memory through sirt1-dependent activation of hippocampal brain-derived neurotrophic factor (BDNF). J Neurosci. 2019;39(13):2369-82. 122. Schiffer T, Schulte S, Sperlich B, Achtzehn S, Fricke H, et al. Lactate infusion at rest increases BDNF blood concentration in humans. Neurosci Lett. 2011;488(3):234-7. 123. Kujach S, Olek RA, Byun K, Suwabe K, Sitek EJ, et al. Acute sprint interval exercise increases both cognitive functions and peripheral neurotrophic factors in humans: the possible involvement of lactate. Front Neurosci. 2019;13:1455. 124. Morland C, Andersson KA, Haugen ØP, Hadzic A, Kleppa L, et al. Exercise induces cerebral VEGF and angiogenesis via the lactate receptor HCAR1. Nature communications. 2017;8(1):15557. 125. Brandner CR, Warmington SA, Kidgell DJ. Corticomotor excitability is increased following an acute bout of blood flow restriction Resistance Exercise. Front Hum Neurosci. 2015;9:652. 126. Morita T, Fukuda T, Kikuchi H, Ikeda K, Yumoto M, et al. Effects of blood flow restriction on cerebral blood flow during a single arm-curl resistance exercise. International Journal of KAATSU Training Research. 2010;6(1):9-12. 127. Sugimoto T, Suga T, Tomoo K, Dora K, Mok E, et al. Blood flow restriction improves executive function after walking. Med Sci Sports Exerc. 2021;53(1):131-8. 128. de Queiros VS, Dantas M, Neto GR, da Silva LF, Assis MG, et al. Application and side effects of blood flow restriction technique: A cross-sectional questionnaire survey of professionals. Medicine (Baltimore). 2021;100(18):e25794. 129. Wong ML, Formiga MF, Owens J, Asken T, Cahalin LP. Safety of blood flow restricted exercise in hypertension: a meta-analysis and systematic review with potential applications in orthopedic care. Techniques in Orthopaedics. 2018;33(2):80-8. 130. Cezar MA, De Sá CA, Corralo VdS, Copatti SL, Santos GAGd, et al. Effects of exercise training with blood flow restriction on blood pressure in medicated hypertensive patients. Motriz: Revista de Educação Física. 2016;22:9-17. 131. Kambič T, Novaković M, Tomažin K, Strojnik V, Božič-Mijovski M, et al. Hemodynamic and hemostatic response to blood flow restriction resistance exercise in coronary artery disease: A Pilot Randomized Controlled Trial. J Cardiovasc Nurs. 2021;36(5):507-16. 132. Lee YG, Park W, Kim SH, Yun SP, Jeong H, et al. A case of rhabdomyolysis associated with use of a pneumatic tourniquet during ar-throscopic knee surgery. Korean J Intern Med. 2010;25(1):105-9. 133. Desai K, Dinh TP, Chung S, Pierpont YN, Naidu DK, et al. Upper extremity deep vein thrombosis with tourniquet use. Int J Surg Case Rep. 2015;6c:55-7. 134. Nakajima T, Kurano M, Iida H, Takano H, Oonuma H, et al. Use and safety of KAATSU training: results of a national survey. International journal of KAATSU training research. 2006;2(1):5-13. 135. Patterson SD, Hughes L, Warmington S, Burr J, Scott BR, et al. Blood flow restriction exercise: Considerations of Methodology, Application, and Safety. Front Physiol. 2019;10:533. 136. Loenneke J, Thiebaud R, Abe T, Bemben M. Blood flow restriction pressure recommendations: the hormesis hypothesis. Medical hypoth-eses. 2014;82(5):623-6. 137. Loenneke JP, Fahs CA, Rossow LM, Thiebaud RS, Mattocks KT, et al. Blood flow restriction pressure recommendations: a tale of two cuffs. Front Physiol. 2013;4:249. 138. McEwen JA, Owens JG, Jeyasurya J. Why is it crucial to use person-alized occlusion pressures in blood flow restriction (BFR) rehabilitation? Journal of Medical and Biological Engineering. 2019;39:173-7. 139. Nakajima T, Morita T, Sato Y. Key considerations when conducting KAATSU training. International Journal of KAATSU Training Research. 2011;7(1):1-6.
|
|